RSNA Press Release
- Partial breast irradiation with brachytherapy offers benefits over total breast irradiation in treating early-stage cancer in some women.
- Ultrasound-guided balloon catheter placement before brachytherapy is minimally invasive.
- The new approach ensures that the patient is a good candidate for brachytherapy before a catheter is placed.
Breast Cancer Treatment Procedure Gives Women More Options
Released: November 29, 2006
| Media Contacts: | ||
| RSNA Media Relations: | (630) 590-7762 | |
| Maureen Morley (630) 590-7754 mmorley@rsna.org |
||
CHICAGO — A new minimally invasive approach to partial breast irradiation provides another treatment option for women with breast cancer. The researchers presented their findings today at the annual meeting of the Radiological Society of North America.
"Women with breast cancer have many serious decisions to make in a short amount of time, including decisions regarding radiation therapy," said Lora D. Barke, D.O., assistant professor at Feinberg School of Medicine, Northwestern University and Northwestern Memorial Hospital in Chicago. "This procedure, which uses ultrasound to precisely guide balloon catheter placement to the lumpectomy site for partial breast irradiation treatment, removes one weighty decision women must make before surgery."
This is the first study to assess the use of ultrasound to guide the placement of the balloon catheter before partial breast irradiation therapy with brachytherapy.
In treatment with breast brachytherapy, the cancerous breast lump is surgically excised, and radiation is directed only to the portion of the breast surrounding the lumpectomy site. This approach maintains the likelihood of destroying the tumor but reduces the risk of damaging healthy tissue far from the tumor site. Since the target is smaller, brachytherapy allows for a shorter treatment regime-averaging five to seven days, compared to conventional whole-breast, external beam radiation, which may take six to seven weeks.
Balloon catheters used to deliver radiation to the affected area with brachytherapy are sometimes placed during surgery, or a surgical incision is reopened to insert the catheter. Often the catheter is placed unnecessarily, because later findings reveal that localized radiation is not appropriate or the breast tissue overlying the balloon is too thin.
"Our research shows that immediate placement of the balloon catheter is unnecessary and may add to cost. Radiologists can wait until receiving the final pathology, and then safely and efficiently insert the catheter with ultrasound guidance immediately before the patient begins brachytherapy," Dr. Barke explained. "This allows time to determine if brachytherapy is appropriate for the patient and allows the patient and physician to consider and weigh the benefits of various treatment options," she said.
The researchers studied ultrasound guidance of balloon catheter placement into the lumpectomy cavities of 75 new patients with early-stage breast cancer seven to 47 days after their lumpectomies. Patients were initially screened to assure an adequate surgical cavity size and skin thickness over the balloon. After successful insertion of the catheter, patients received twice-a-day brachytherapy treatments for one week.
The investigators concluded that ultrasound-guided placement of partial breast irradiation balloon catheters is safe, efficient and minimally invasive. No immediate complications occurred at insertion. One balloon ruptured and had to be replaced. Insertion of the catheter with local anesthesia took less than five minutes. The total procedure, including preparation time, averaged 25 minutes.
Co-authors are Ellen B. Mendelson, M.D., Krystyna D. Kiel, M.D., and Judith A. Wolfman, M.D.
# # #
RSNA is an association of more than 40,000 radiologists, radiation oncologists, medical physicists and related scientists committed to promoting excellence in radiology through education and by fostering research, with the ultimate goal of improving patient care. The Society is based in Oak Brook, Ill.
Editor's note: The data in these releases may differ from those in the printed abstract and those actually presented at the meeting, as researchers continue to update their data right up until the meeting. To ensure you are using the most up-to-date information, please call the RSNA Newsroom at (312) 949-3233.
| Abstract: |
Images (.JPG format)
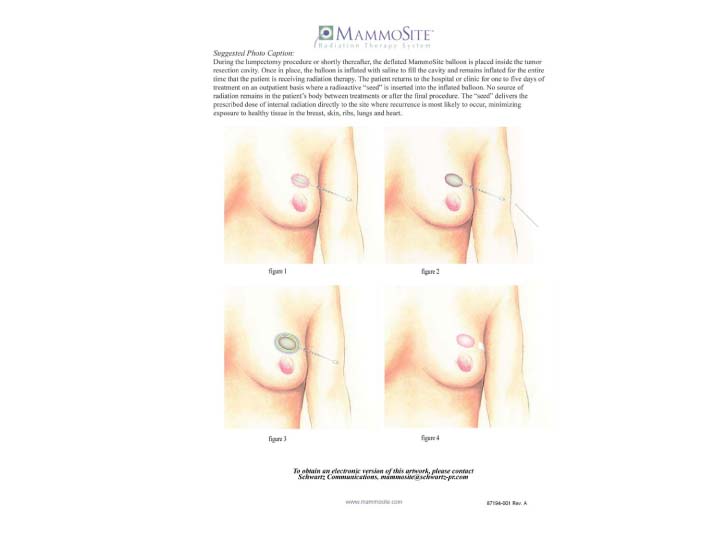 Figure 1. During the lumpectomy procedure or shortly thereafter, the deflated MammoSite balloon is placed inside the tumor resection cavity. Once in place, the balloon is inflated with saline to fill the cavity and remains inflated for the entire time that the patient is receiving radiation therapy. The patient returns to the hospital or clinic for one to five days of treatment on an outpatient basis where a radioactive "seed" is inserted into the inflated balloon. No source of radiation remains in the patient's body between treatments or after the final procedure. The "seed" delivers the prescribed does of internal radiation directly to the site where recurrence is most likely to occur, minimizing exposure to healthy tissue in the breast, skin, ribs, lungs, and heart. High-res (TIF) version (Right-click and Save As) |
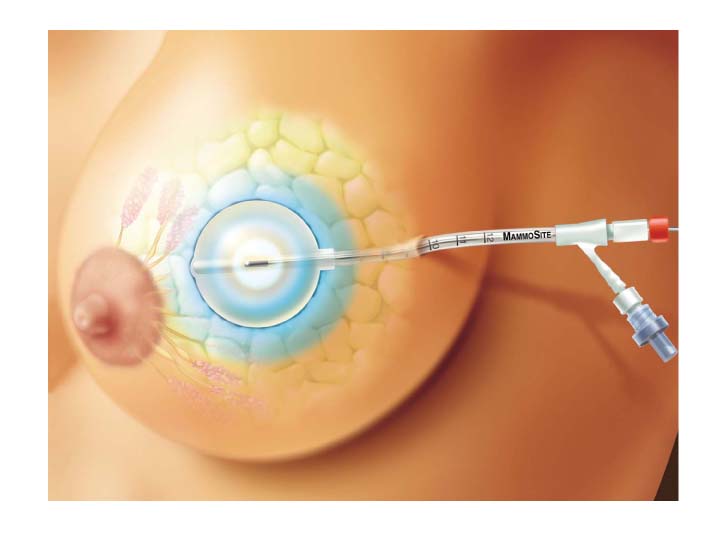 Figure 2. Illustration of MammoSite balloon inside tumor resection cavity. High-res (TIF) version (Right-click and Save As) |
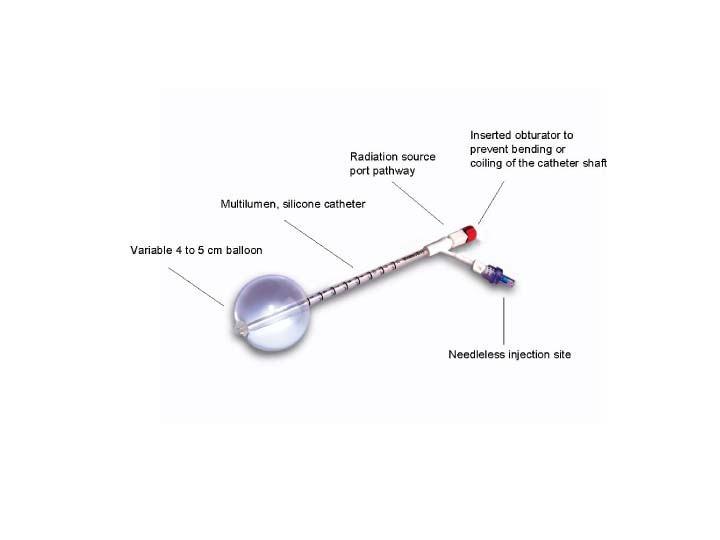 Figure 3. MammoSite equipment diagram with labels. High-res (TIF) version (Right-click and Save As) |
|
 Figure 4. Ultrasound-guided breast brachytherapy procedure High-res (TIF) version (Right-click and Save As) |
 Figure 5. Ultrasound-guided breast brachytherapy procedure High-res (TIF) version (Right-click and Save As) |
 Figure 6. Ultrasound-guided breast brachytherapy procedure High-res (TIF) version (Right-click and Save As) |
 Figure 7. Ultrasound-guided breast brachytherapy procedure High-res (TIF) version (Right-click and Save As) |
 Figure 8. Ultrasound-guided breast brachytherapy procedure High-res (TIF) version (Right-click and Save As) |
|||
 PDF
PDF