RSNA Press Release
- Magnetic resonance-guided focused ultrasound surgery (MRgFUS) safely and effectively treats fibroids in women.
- MRgFUS significantly relieves uterine fibroid symptoms and reduces fibroid volume.
- Fibroids affect approximately 25 percent of women in their reproductive years and account for one-third of the hysterectomies performed annually in the United States.
Noninvasive Ultrasound Treatment Shrinks Fibroids
Released: November 30, 2005
| Media Contacts: | |
| RSNA Media Relations: | (630) 590-7762 |
| Maureen Morley (630) 590-7754 mmorley@rsna.org |
Heather Babiar (630) 590-7738 hbabiar@rsna.org |
CHICAGO - A totally noninvasive procedure using high-intensity ultrasound waves to heat and destroy uterine fibroid tissue significantly relieves fibroid-related symptoms in women, according to the results of a multicenter clinical trial. Magnetic resonance-guided, focused ultrasound surgery (MRgFUS) allows radiologists to precisely target fibroids without harming healthy surrounding tissue. The study was presented today at the annual meeting of the Radiological Society of North America (RSNA).
"This treatment immediately stops blood flow in the fibroid tissue, which results in a significant, sustained decrease in symptoms for up to 12 months," said the study's lead author, Fiona M. Fennessy, M.D., Ph.D., instructor of radiology at Harvard Medical School and staff radiologist at Brigham and Women's Hospital in Boston.
Uterine fibroids are benign growths of the muscle inside the uterus. According to the National Institutes of Health, at least 25 percent of women in the United States age 25 to 50 suffer from uterine fibroids, and as many as 50 percent of African American women have uterine fibroids.
Symptoms can include excessive menstrual bleeding, enlarged uterine size, frequent urination, pelvic pressure or pain and infertility. The absolute treatment for symptomatic fibroids is hysterectomy, which is the complete removal of the uterus. According to the National Women's Health Information Center, fibroids are the primary reason for hysterectomy, accounting for 175,000, or approximately one-third, of hysterectomies performed annually in the United States.
"Hysterectomy is currently the gold standard of therapy for uterine fibroids," Dr. Fennessy said. "However, women are increasingly seeking minimally invasive or noninvasive alternatives to hysterectomy."
Dr. Fennessy and colleagues studied 160 women with symptomatic fibroids treated as part of a clinical trial at five medical centers. The women received pre-treatment MR imaging to identify and define the target fibroids for MRgFUS. Radiologists then used focused ultrasound to deliver heat to the targeted fibroid volume. Temperature-sensitive MR guidance allowed the team to monitor the location of the ultrasound beam and to track temperature changes in tissue during the procedure.
One hundred eleven patients were treated under the original study protocol (A), and 51 patients were treated under an optimized protocol (B). Protocol A allowed a maximum treatment time of 120 minutes or a maximum treatment volume of 100ccs (roughly six centimeters (cm) in diameter), or up to 33 percent of total fibroid volume. Protocol B allowed a maximum treatment time of 180 minutes and maximum treatment volume of 150ccs (about 7 cm in diameter), or up to 33 percent of total volume in subserosal fibroids (those on the outer wall of the uterus) and 50 percent of volume in non-subserosal fibroids.
Treatment outcomes were assessed by Uterine Fibroids Symptoms and Quality of Life (UFSQOL) scores obtained at baseline, three, six and 12 months post-treatment. The findings showed significant symptom relief at three and six months and sustained relief at one year. Women treated with the optimized protocol reported greater symptom relief and quality of life improvement than those treated with the original protocol. No serious adverse effects were reported. Initial findings in follow-up of patients 24 and 36 months after treatment suggest that symptom relief is maintained.
"We have shown that treating fibroids with an optimized, less restrictive protocol allows for treatment of a greater fibroid volume, which results in even greater symptomatic relief at clinical follow-up," Dr. Fennessy said.
Co-authors are Clare M. Tempany, M.D., Kelly H. Zou, Ph.D., Minna J. So, M.D., Elizabeth A. Stewart, M.D., Frank J. Rybicki, M.D., Ph.D., Nathan J. McDannold, Ph.D., Kullervo Hynynen, Ph.D., Gina K. Hesley, M.D., and Ferenc A. Jolesz, M.D.
# # #
Note: Copies of RSNA 2005 news releases and electronic images will be available online at RSNA.org/press05 beginning Monday, Nov. 28.
RSNA is an association of more than 38,000 radiologists, radiation oncologists, medical physicists and related scientists committed to promoting excellence in radiology through education and by fostering research, with the ultimate goal of improving patient care. The Society is based in Oak Brook, Ill.
Editor's note: The data in these releases may differ from those in the printed abstract and those actually presented at the meeting, as researchers continue to update their data right up until the meeting. To ensure you are using the most up-to-date information, please call the RSNA Newsroom at (312) 949-3233.
| Abstract: |
Video clips
- .AVI format
- Video clip 1 (8,173 Kbyte)
- .WMV format
- Video clip 2 (1,488 Kbyte)
Images (.JPG format)
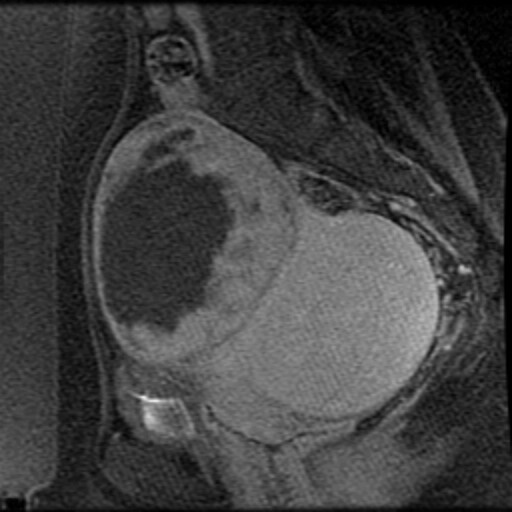
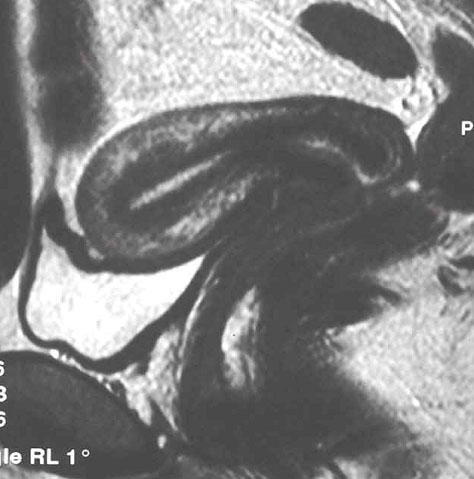 Figure 1. MR image of uterine fibroids. |
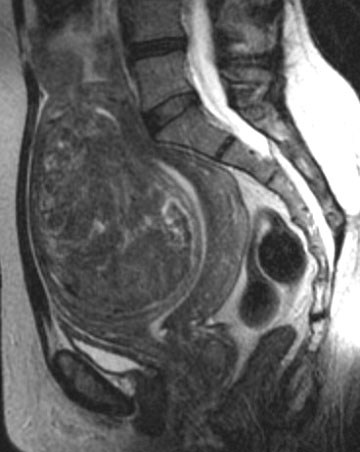 Figure 2. MR image of uterine fibroids. |
 Figure 3. Examples of surgical equipment used in traditional uterine fibroid treatments. |
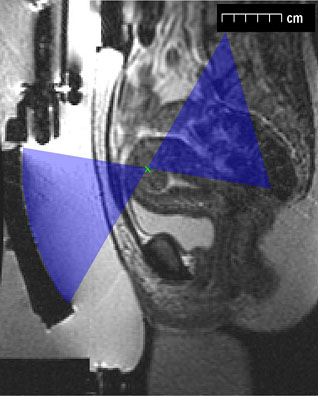 Figure 4. MR image pinpointing the location of a woman's uterine fibroids. |
 Figure 5. A patient going into magnetic resonance imaging equipment. |
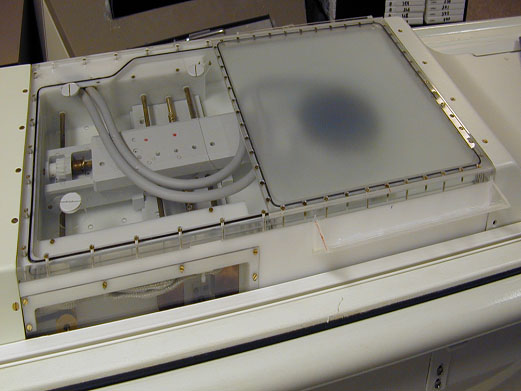 Figure 6. MRgFUS equipment. |
 Figure 7. MR imaging of a woman undergoing treatment for uterine fibroids. The high intensity ultrasound waves heat and kill target tissue. Magnetic resonance directs the ultrasound beam and monitors heating in tissue. |
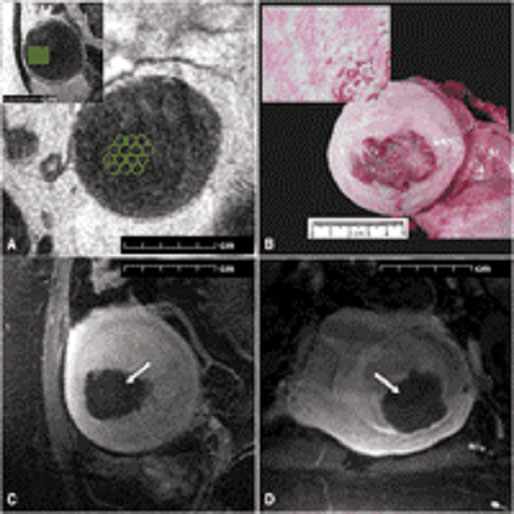 Figure 8. MR images of uterine fibroids, treatment planning and treatment. |
 Figure 9. MR image of uterine fibroids before MRgFUS. |
 Figure 10. MR image of uterine fibroids immediately after MRgFUS. The greater the fibroid volume treated, the better the outcome. |
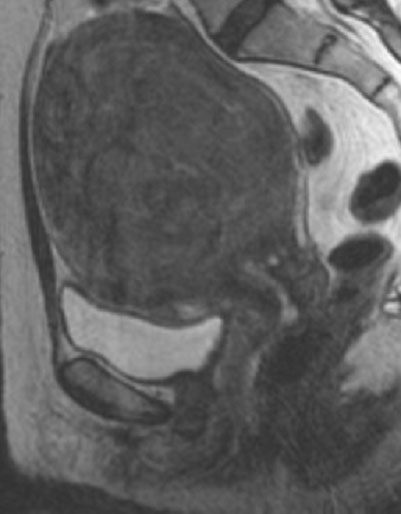 Figure 11. MR image of uterine fibroids before MRgFUS. |
 Figure 12. MR image of uterine fibroids one year after MRgFUS. |
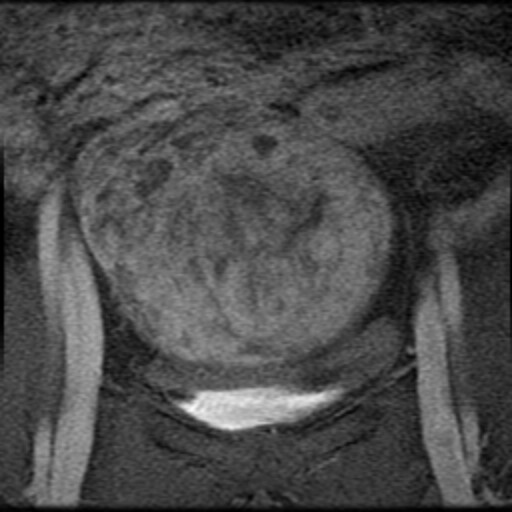
 Case 1a. Axial T1 post-gadolinium, immediately post-treatment demonstrating a large area of non-enhancement, consistent with treatment effect. High-res (TIF) version (Right-click and Save As) |
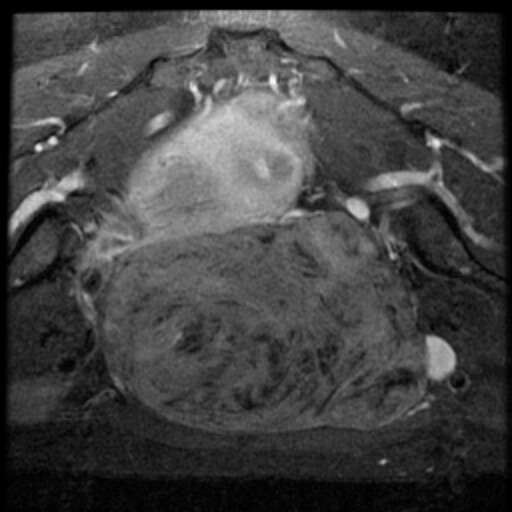 Case 1b. Axial T1 post-gadolinium, taken prior to treatment demonstrating enhancement of the uterine fibroid. High-res (TIF) version (Right-click and Save As) |
 Case 1c. Coronal T1 post-gadolinium, immediately post-treatment demonstrating a large area of non-enhancement, consistent with treatment effect. High-res (TIF) version (Right-click and Save As) |
 Case 1d. Coronal T1 post-gadolinium, taken prior to treatment demonstrating enhancement of the uterine fibroid. High-res (TIF) version (Right-click and Save As) |
 Case 1e. Sagittal T1 post-gadolinium, immediately post-treatment demonstrating a large area of non-enhancement, consistent with treatment effect. High-res (TIF) version (Right-click and Save As) |
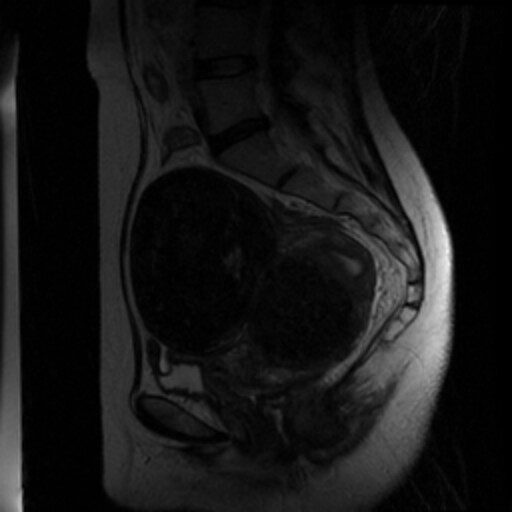 Case 1f. Sagittal T2 pre-treatment outlining the uterine fibroid, taken prior to treatment. High-res (TIF) version (Right-click and Save As) |
||
| Case 1 figures a, c and e are axial, coronal and sagittal of the same finding, post-treatment.
Case 1 figures b, d and f and axial, coronal and sagittal of the same finding, pre-treatment. | |||
 PDF
PDF