Ultra-Low Dose CT Aids Pneumonia Diagnosis in Immunocompromised Patients
Released: March 13, 2025
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org
OAK BROOK, Ill. — Denoised ultra-low dose CT can effectively diagnose pneumonia in immunocompromised patients using only 2% of the radiation dose of standard CT, according to a study published today in Radiology: Cardiothoracic Imaging, a journal of the Radiological Society of North America (RSNA).

“For patients with weakened immune systems, lung infections can be life threatening,” said lead study author Maximiliano Klug, M.D., a radiologist in the division of diagnostic imaging at the Sheba Medical Center in Ramat Gan, Israel. “CT scans are the gold standard for detecting pneumonia, but repeated scans can expose patients to significant radiation.”
While the early diagnosis of lung infections in immunocompromised patients is important, the risks of cumulative radiation dose exposure from frequent CT scans is a concern.
Ultra-low dose CT reduces radiation exposure but can result in poor image quality due to added “noise,” which manifests as a grainy texture throughout the image. This reduction in image quality can affect the accuracy of diagnosis. Therefore, Dr. Klug and colleagues sought to test the denoising capabilities of a deep learning algorithm on ultra-low dose CT scans.
From September 2020 to December 2022, 54 immunocompromised patients with fevers were referred to Dr. Klug’s division to undergo two chest CT scans: a normal dose scan and an ultra-low dose scan. A deep learning algorithm was applied to denoise all 54 of the ultra-low dose CT scans.
Radiologists individually assessed and documented their findings from the normal dose CT, ultra-low dose CT and denoised ultra-low dose CT scans. They were blinded to all patient clinical information.
The deep learning algorithm significantly improved the image quality and clarity of the ultra-low dose CT scans and reduced false positives. Nodules were also more easily identified on the denoised scans.
The average effective radiation dose for ultra-low dose scans was 2% of the average effective radiation dose of the standard CT scans.
“This study paves the way for safer, AI-driven imaging that reduces radiation exposure while preserving diagnostic accuracy,” Dr. Klug said.
The researchers note that deep learning-based denoising on ultra-low dose CT scans can be beneficial in other patient groups, such as young patients.
“This pilot study identified infection with a fraction of the radiation dose,” Dr. Klug said. “This approach could drive larger studies and ultimately reshape clinical guidelines, making denoised ultra-low dose CT the new standard for young immunocompromised patients.”
Future studies with larger sample sizes will help validate the findings from this study.
“Denoised Ultra-Low-Dose Chest CT to Assess Pneumonia in Individuals Who Are Immunocompromised Individuals.” Collaborating with Dr. Klug were Tamer Sobeh, M.D., Michael Green, M.Sc., Arnaldo Mayer, Ph.D., Zehavit Kirshenboim, M.D., Eli Konen, M.D., and Edith Michelle Marom, M.D.
Radiology: Cardiothoracic Imaging is edited by Suhny Abbara, M.D., University of Texas Southwestern Medical Center, Dallas, and owned and published by the Radiological Society of North America, Inc.(https://pubs.rsna.org/journal/cardiothoracic)
RSNA is an association of radiologists, radiation oncologists, medical physicists and related scientists promoting excellence in patient care and health care delivery through education, research, and technologic innovation. The Society is based in Oak Brook, Illinois. (RSNA.org)
For patient-friendly information on chest CT, visit RadiologyInfo.org.
Images (JPG, TIF):
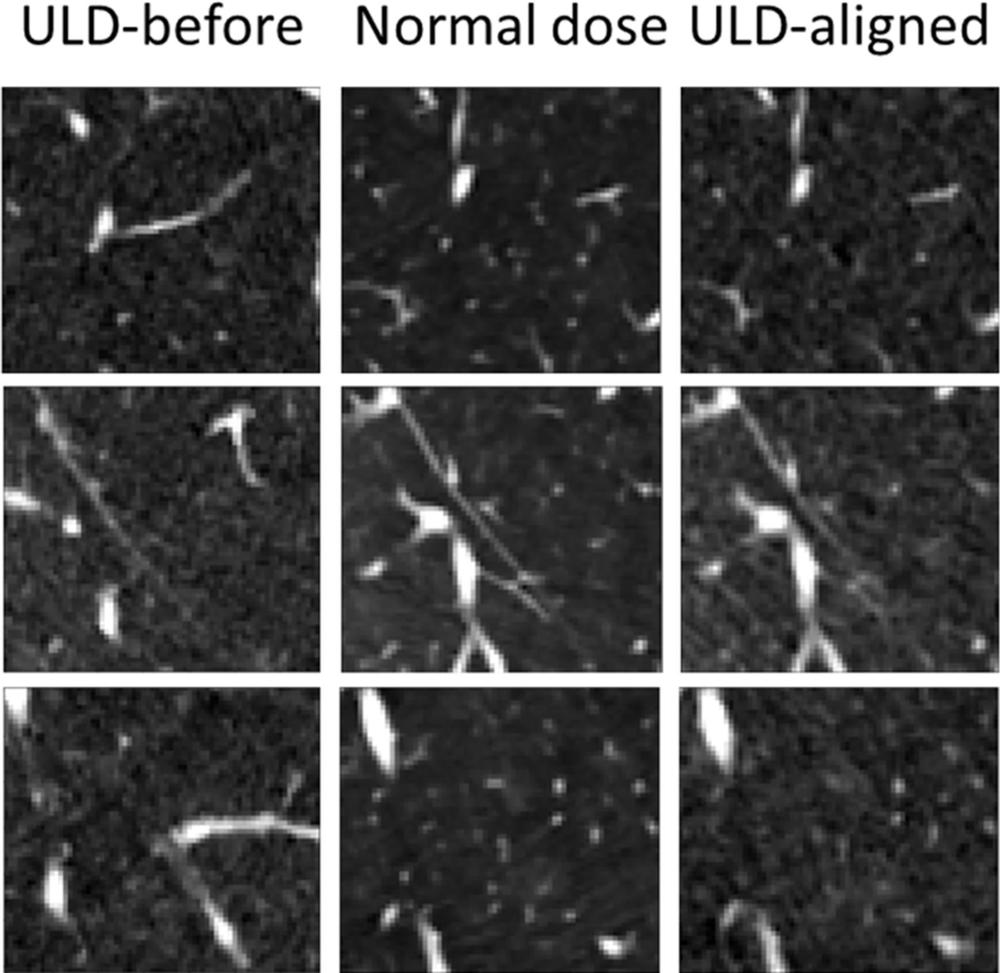
Figure 1. Axial noncontrast chest CT lung window images of three different sample patches shown in each row. Ultra-low-dose [ULD] patches before alignment (left column) are clearly misaligned to the normal-dose patches (middle column). After alignment (right column), the spatial misalignment is mostly compensated.
High-res (TIF) version
(Right-click and Save As)
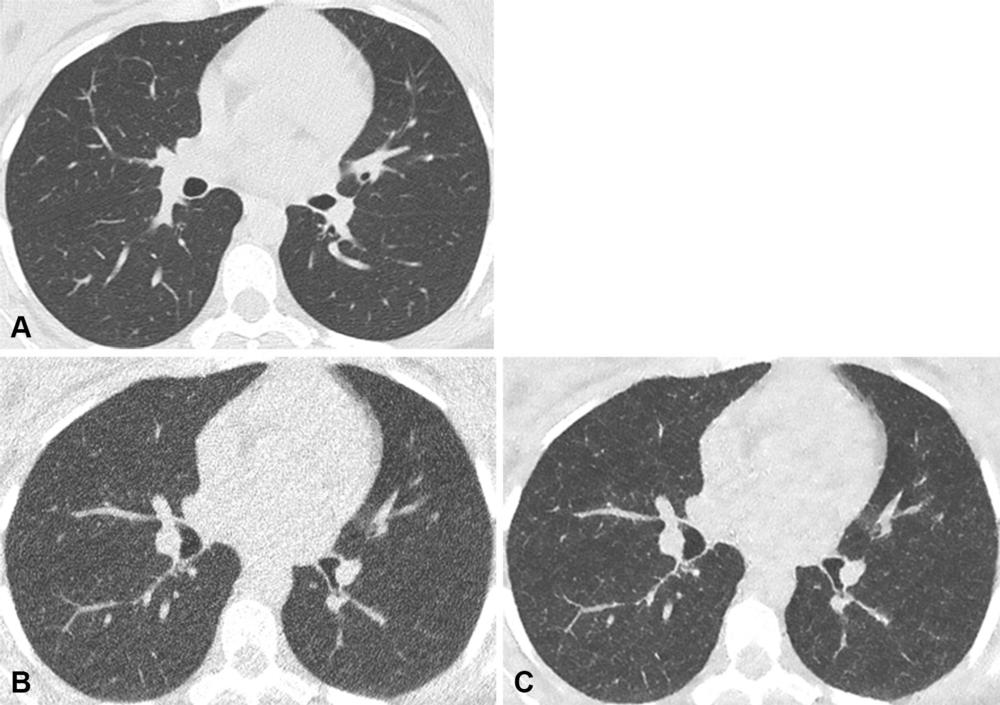
Figure 2. Axial noncontrast chest CT lung window images in a 42-year-old male participant with normal lungs. (A) Normal-dose CT, (B) ultra-low-dose CT (ULDCT), and (C) denoised ULDCT images. Normal lungs were observed on normal-dose CT image. However, due to inherent image noise at ULDCT, the lung pattern was falsely classified as positive viral infection by both readers. The denoising technique of the denoised ULDCT corrected this artifact, and the participant was correctly categorized as having no infection.
High-res (TIF) version
(Right-click and Save As)
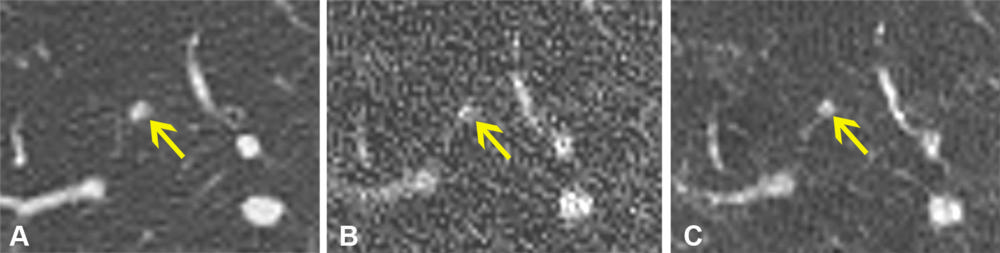
Figure 3. Axial noncontrast chest CT lung window images in a 54-year-old female participant. (A) Normal-dose CT, (B) ultra-low-dose CT (ULDCT), and (C) denoised ULDCT images show a solid lung small nodule of less than 1 cm (yellow arrow). A solid nodule was observed on normal-dose CT image. However, image noise at ULDCT precluded the correct classification, and the nodule was identified as part solid by both readers. Denoised ULDCT reduced the image noise, allowing correct classification as a solid nodule.
High-res (TIF) version
(Right-click and Save As)
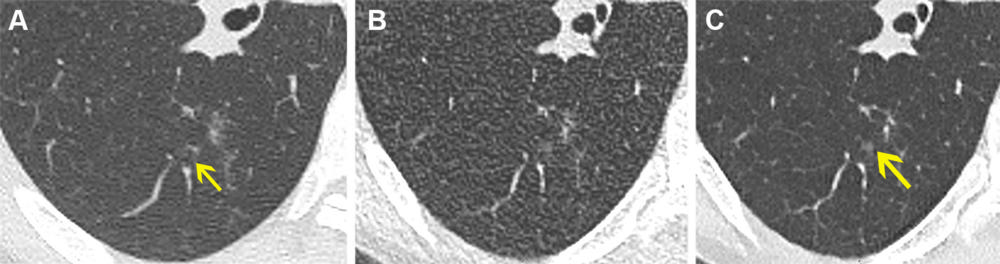
Figure 4. Axial noncontrast chest CT lung window images in a 61-year-old female participant. (A) Normal-dose CT, (B) ultra-low-dose CT (ULDCT), and (C) denoised ULDCT show focal ground-glass opacity (yellow arrow). Ground-glass opacity was correctly identified with both normal- dose CT and denoised ULDCT, but it was missed by both readers at ULDCT due to decreased signal-to-noise ratio.
High-res (TIF) version
(Right-click and Save As)
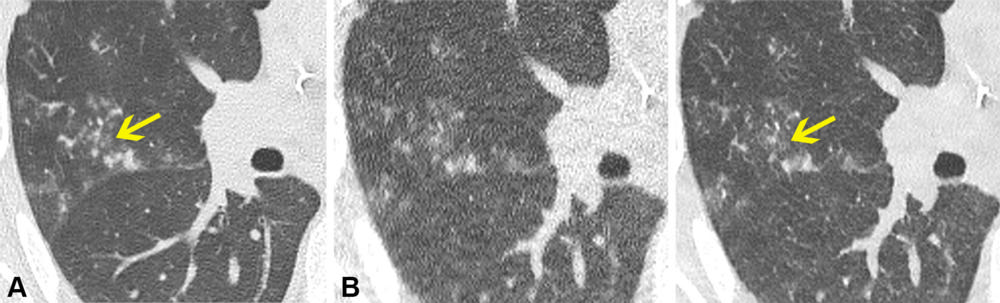
Figure 5. Axial noncontrast chest CT lung window images in a 70-year-old male participant. (A) Normal-dose CT, (B) ultra-low-dose CT (ULDCT), and (C) denoised ULDCT images show tree-in-bud opacities (yellow arrow). The tree-in-bud opacities can be observed on normal-dose CT image. However, due to the increased image noise at ULDCT, the linear branching pattern was missed and classified incorrectly by both readers as nodules with no tree-in-bud opacities. Denoised ULDCT allowed better appreciation of centrilobular nodules with a linear branching pattern, and the image was classified correctly as positive for tree-in-bud opacities.
High-res (TIF) version
(Right-click and Save As)
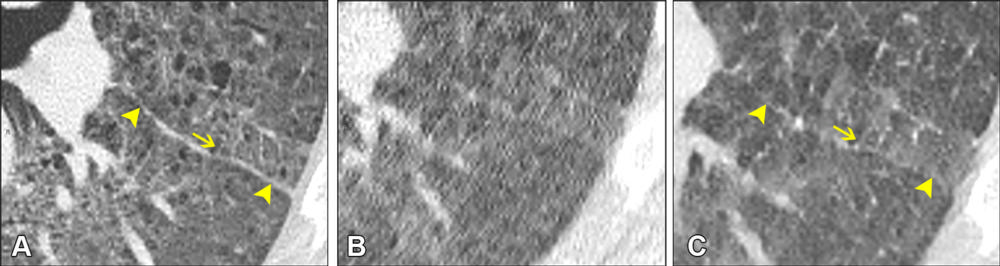
Figure 6. Axial noncontrast chest CT lung window images in a 65-year-old male participant. (A) Normal-dose CT, (B) ultra-low-dose CT (ULDCT), and (C) denoised ULDCT images show interlobular septal thickening (yellow arrow pointing to one of them) forming a 90° angle with the fissure (arrowheads). Interlobular septal thickening can be clearly visualized on normal-dose CT image. However, both readers failed to detect this finding on the ULDCT image due to increased image noise. Denoised ULDCT corrected the artifact, allowing for detection of interlobular septal thickening by the readers.
High-res (TIF) version
(Right-click and Save As)