Lung Nodules Seen in a High Percentage of Non-Smokers
Released: August 13, 2024
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Imani Harris
1-630-481-1009
iharris@rsna.org
OAK BROOK, Ill. — A new study of more than 10,000 non-smoking adults found that solid lung nodules were present in a considerable portion of study participants. Non-smokers are traditionally thought to be at low risk for lung nodules and lung cancer. The results of the study were published today in Radiology, a journal of the Radiological Society of North America (RSNA).
Incidental lung nodules are common findings on chest CT and in high-risk groups are more likely to be a sign of early-stage lung cancer. Because most previous research on the prevalence and size of lung nodules has typically been derived from lung cancer screening studies in heavy smokers, nodule management recommendations are mostly based on this patient population. Thus, our current nodule follow-up guidelines which are mostly based on high-risk patient populations may lead to many unnecessary follow-up examinations in low-risk individuals with incidental pulmonary nodules.

"This study is groundbreaking as it provides the first comprehensive analysis of the prevalence and size distribution of solid lung nodules in a population-based Northern European non-smoking cohort," said senior author Rozemarijn Vliegenthart, M.D., Ph.D., radiologist and professor of cardiothoracic imaging at the University Medical Center Groningen and the University of Groningen in the Netherlands. "Unlike prior studies that predominantly targeted high-risk lung cancer screening cohorts or Asian cohorts, this research yields fundamental data for the general non-smoking population in northern Europe."
The study included 10,431 never- or former smokers aged 45 and over from the Imaging in LifeLines (ImaLife) study, the first population-based imaging study designed to establish the reference values of imaging biomarkers for early stages of coronary artery disease, lung cancer and chronic obstructive pulmonary disease in a general population of mostly non-smokers.
Of the participants in the current study, 56.6% were women (median age 60.4 years), 46.1% were never smokers and 53.9% were former smokers.
"By including a large cohort of non-smoking men and women aged 45 years and above, this research offers insights into the prevalence and characteristics of lung nodules in a population group that has not been studied before," Dr. Vliegenthart said.
Participants underwent a low-dose CT exam of the chest. Seven trained readers registered the presence and size of solid lung nodules. Along with the prevalence and size of the lung nodules, they noted clinically relevant and actionable nodules.
At least one lung nodule was found in 4,377 (42.0%) of the participants (47.5% of men; 37.7% of women). The prevalence of lung nodules increased with age. Clinically relevant lung nodules (nodules measuring 6 to 8 mm) were present in 11.1% of participants, with the prevalence again increasing with age. Men were more likely than women to have lung nodules, and men were more likely than women to have multiple nodules.
"Our study revealed the presence of clinically relevant nodules in 11.1 percent of a non-smoking cohort, traditionally considered low risk," Dr. Vliegenthart said. "This was higher than we expected and even similar to the prevalence reported in high-risk populations of smokers."
In recent years, the proportion of smoking individuals in Western populations has been declining due to the success of smoking cessation programs, Dr. Vliegenthart noted.
"This shift makes our study, which provides foundational and comprehensive data on lung nodules in non-smokers, even more critical," she said.
The results imply that, given the increasing numbers of chest CT scans for various clinical indications, these incidental nodules will increase the number of follow-up scans and workups when using current nodule follow-up guidelines. As the patients are followed in the LifeLines cohort over time, we can gather more data to determine if lower risk patient population may need altered follow-up management.
"We know that the incidence of lung cancer in this population (LifeLines cohort), is very low (0.3%), suggesting that most of the clinically relevant and even actionable nodules in a non-smoking cohort are benign," Dr. Vliegenthart said. "Future data on lung cancer diagnosis in ImaLife participants with clinically relevant and actionable nodules may help to optimize nodule management recommendations for individuals considered at low risk."
"Distribution of Solid Lung Nodules Presence and Size by Age and Sex in a Northern European Nonsmoking Population." Collaborating with Dr. Vliegenthart were Jiali Cai, M.D., Marleen Vonder, Ph.D., Gert Jan Pelgrim, Ph.D., Mieneke Rook, M.D., Ph.D., Gerdien Kramer, M.D., Ph.D., Harry J.M. Groen, M.D., Ph.D., and Geertruida H. de Bock, Ph.D.
Radiology is edited by Linda Moy, M.D., New York University, New York, N.Y., and owned and published by the Radiological Society of North America, Inc. (https://pubs.rsna.org/journal/radiology)
RSNA is an association of radiologists, radiation oncologists, medical physicists and related scientists promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Illinois. (RSNA.org)
For patient-friendly information on chest CT and lung cancer screening, visit RadiologyInfo.org.
Images (JPG, TIF):
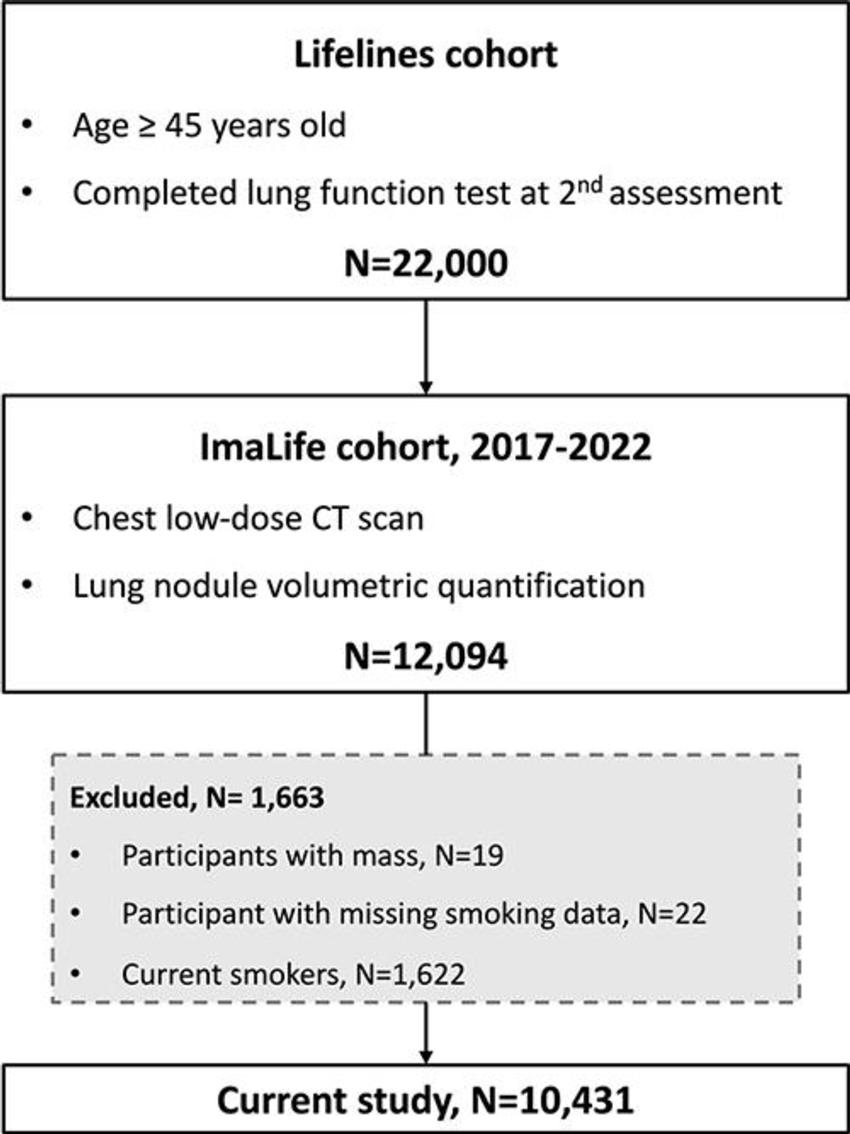
Figure 1. Flowchart of the Imaging in Lifelines (ImaLife) study.
High-res (TIF) version
(Right-click and Save As)
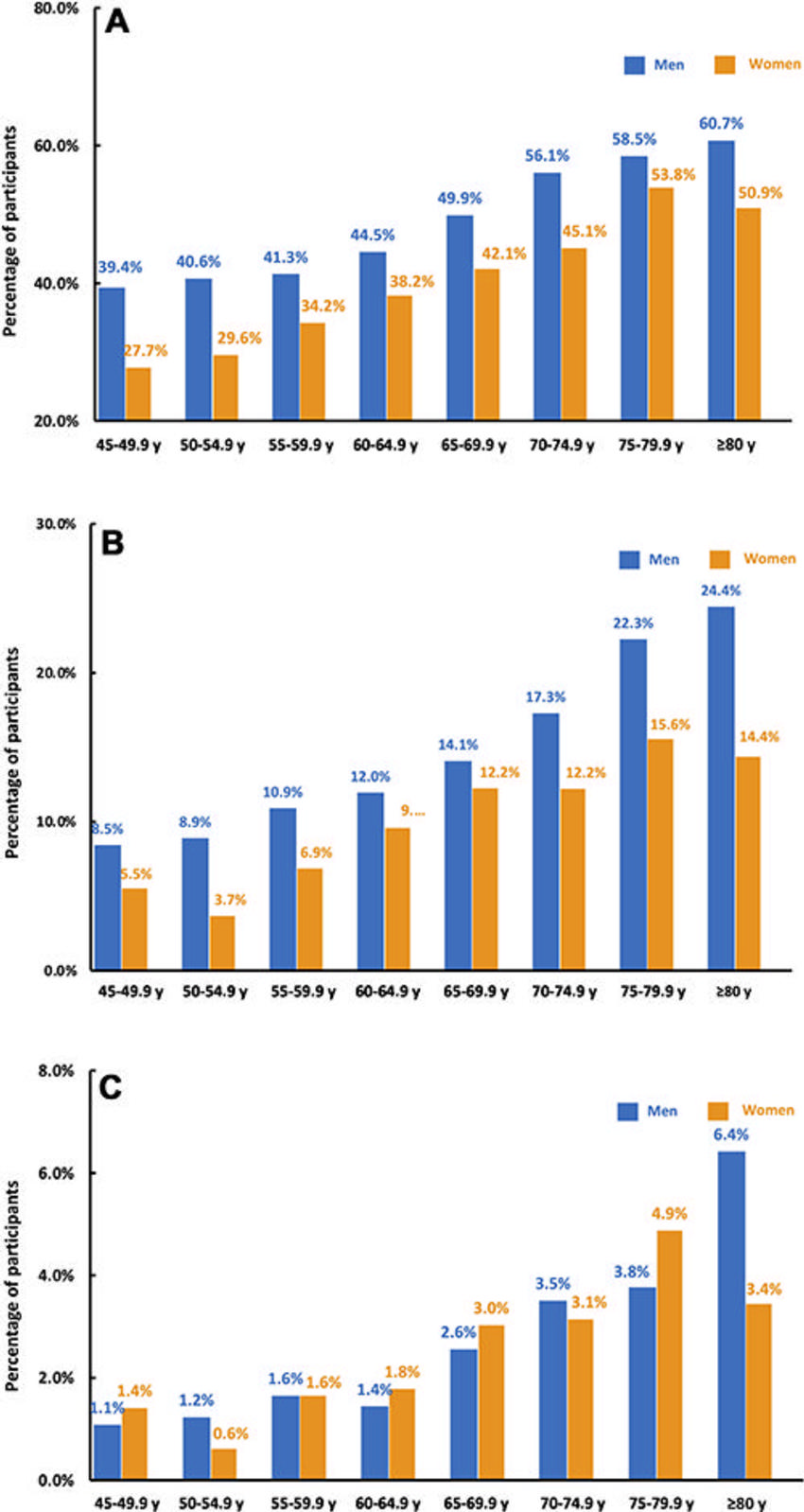
Figure 2. Bar graphs of (A) general prevalence of solid lung nodules (≥30 mm3), (B) clinically relevant lung nodules (≥100 mm3), and (C) actionable lung nodules (≥300 mm3) among participants across age categories.
High-res (TIF) version
(Right-click and Save As)
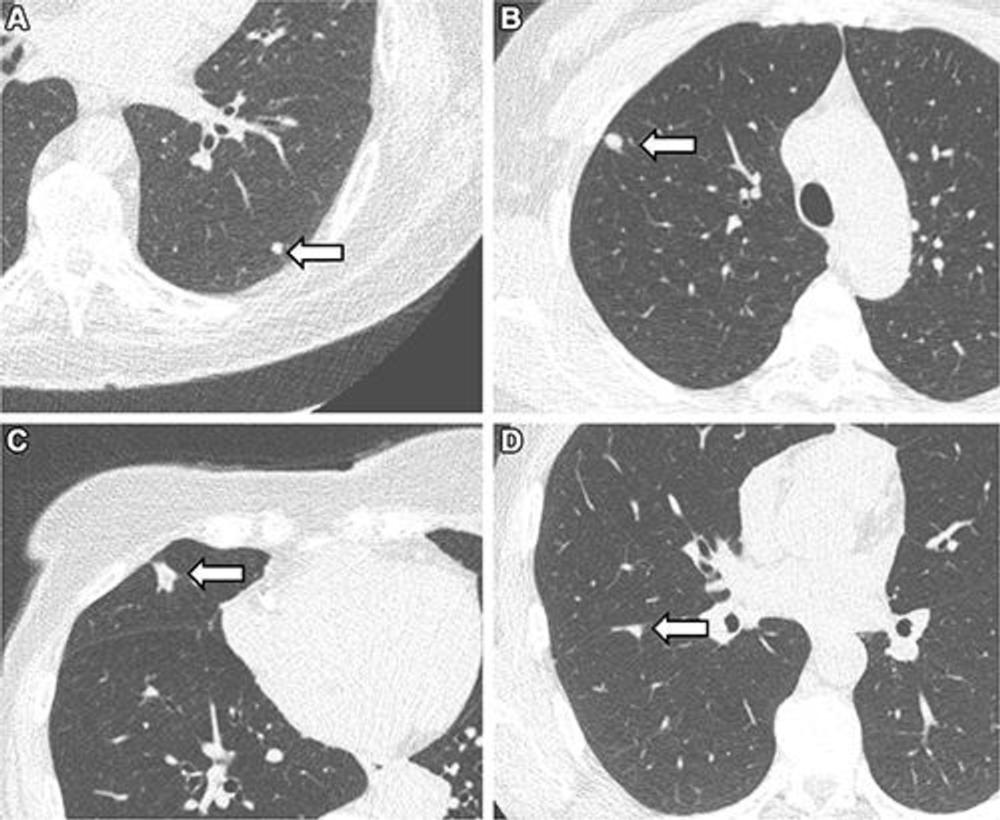
Figure 3. Representative chest low-dose CT images show lung nodules (arrows) and were included in the study. (A) A solid lung nodule, 82 mm3, in a 77-year-old male participant. (B) A clinically relevant nodule, 174 mm3, in a 55-year-old female participant. (C) An actionable nodule, 422 mm3, in a 79-year-old female participant. (D) A typical perifissural nodule, 183 mm3, in a 46-year-old male participant.
High-res (TIF) version
(Right-click and Save As)