CT Test Simulates Blood Flow to Assess Risk in Patients with Angina
Released: September 12, 2023
At A Glance
- Individuals with stable angina and normal coronary blood flow on CT-FFR had a reduced risk of three-year adverse outcomes.
- CT angiography is the first step in identifying coronary artery disease, but it doesn’t show the impact on coronary blood flow.
- CT-FFR provides a precise estimate for coronary blood flow, thereby reducing the need for invasive heart catheterization.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Imani Harris
1-630-481-1009
iharris@rsna.org
OAK BROOK, Ill. — An advanced CT test can identify individuals with stable angina at a reduced risk of three-year adverse outcomes despite their having a high coronary artery calcium score, according to a study published today in Radiology, a journal of the Radiological Society of North America (RSNA).

In the prospective study, researchers in Denmark assessed the three-year clinical outcomes of patients who underwent CT angiography and CT angiography-derived fractional flow reserve (CT-FFR). CT-FFR uses coronary CT angiography images of the heart, AI algorithms and computational fluid dynamics to simulate the amount of blood flowing through the coronary arteries.
“CT angiography is the first step in identifying the presence of coronary artery disease, but it doesn’t show the impact on blood flow in the arteries,” said lead researcher Kristian T. Madsen, M.D., and Ph.D. candidate in the Department of Cardiology at the University Hospital of Southern Denmark in Esbjerg. “Turbulent blood flow may create abnormal pressure in the vessel that grinds down coronary plaques making them prone to rupture.”
Non-contrast enhanced cardiac CT is typically performed prior to CT angiography to determine the amount of coronary artery calcium, which is a surrogate marker for total coronary plaque, a fatty buildup in the arteries, that can lead to a future heart attack. A coronary artery calcium score of 400 or higher indicates high plaque levels. As calcium absorbs a lot of x-rays, it can be especially challenging to assess coronary CT images of patients with high amounts of coronary artery calcium.
The study group included patients with new onset stable coronary artery disease consecutively enrolled in the Assessing Diagnostic Value of Non-Invasive CT-FFR in Coronary Care (ADVANCE) clinical trial between December 2015 and October 2017 at three Danish sites. Eligibility factors for the trial included at least one coronary artery stenosis, or narrowing, greater than 30% and no atrial fibrillation (irregular heartbeat) or prior coronary revascularization, which is a procedure or surgery that improves blood flow to the heart.
Of the 900 participants, 523 had normal CT-FFR results (mean age 64, 318 males) and 377 had abnormal CT-FFR results (mean age 65, 264 males). In the normal results group, the rate of three-year adverse outcomes (defined as all-cause deaths and non-fatal myocardial infarction) was 2.1% (11/523). In the abnormal results group, the rate of three-year adverse outcomes was 6.6% (25/377).
Among the participants with normal CT-FFR results and a high coronary artery calcium score, the three-year adverse outcome rate was 2.2% (4/182). Participants with a high coronary artery calcium score and abnormal CT-FFR results had a 9% (19/212) three-year adverse outcome rate.
“Our study provides evidence for the prognostic potential of CT-FFR in patients with high coronary artery calcium scores,” he said. “Regardless of the patient’s baseline risk and extent of coronary artery disease measured by coronary artery calcium, if CT-FFR results are normal, the prognosis is good.”
According to Dr. Madsen, imaging options to assess the impact of coronary artery disease on blood-flow have different strengths and weaknesses. He said CT-FFR exhibits high diagnostic performance, and its results correlate well with invasively measured fractional flow reserve, an invasive procedure that measures blood flow directly within the coronary arteries.
“In my opinion, CT-FFR is the best option because it provides a blood-flow estimate similar to what you would obtain if you performed invasive heart catheterization,” he said. “You get a reliable and quick answer without performing additional tests or putting the patient through an invasive procedure.”
Dr. Madsen said CT-FFR will allow clinicians to divide the coronary artery disease patient population by risk level and focus on improving the prognosis of high-risk patients.
“CT-FFR provides diagnostic and prognostic information beyond what can be obtained from CT angiography alone across a wide range of coronary artery calcium levels,” he said. “It’s a tool that offers a lot of exciting prospects for the future.”
“Prognostic Value of Coronary CT Angiography-derived Fractional Flow Reserve on 3-year Outcomes in Patients with Stable Angina.” Collaborating with Dr. Madsen were Bjarne L. Nørgaard, M.D., D.M.Sc., Kristian A. Øvrehus, M.D., Ph.D., Jesper M. Jensen, M.D., Ph.D., Erik Parner, M.Sc., Ph.D., Erik L. Grove, M.D., Ph.D., Timothy A. Fairbairn, M.D., Ph.D., Koen Nieman, M.D., Ph.D., Manesh R. Patel, M.D., Campbell Rogers, M.D., Sarah Mullen, M.B.T., Hans Mickley, M.D., D.M.Sc., Allan Rohold, M.D., Ph.D., Hans Erik Bøtker, M.D., D.M.Sc., Jonathon Leipsic, M.D., and Niels Peter R. Sand, M.D., Ph.D.
In 2023, Radiology is celebrating its 100th anniversary with 12 centennial issues, highlighting Radiology’s legacy of publishing exceptional and practical science to improve patient care.
Radiology is edited by Linda Moy, M.D., New York University, New York, N.Y., and owned and published by the Radiological Society of North America, Inc. (https://pubs.rsna.org/journal/radiology)
RSNA is an association of radiologists, radiation oncologists, medical physicists and related scientists promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Illinois. (RSNA.org)
For patient-friendly information on coronary CT, visit RadiologyInfo.org.
Images (JPG, TIF):
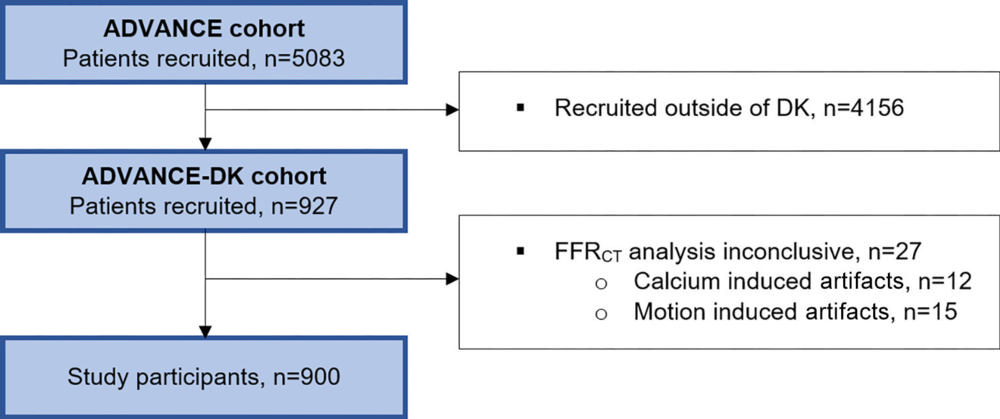
Figure 1. Flow diagram of participant selection. ADVANCE = Assessing Diagnostic Value of Noninvasive CT-FFR in Coronary Care, DK = Denmark, FFRCT = coronary CT angiography–derived fractional flow reserve.
High-res (TIF) version
(Right-click and Save As)
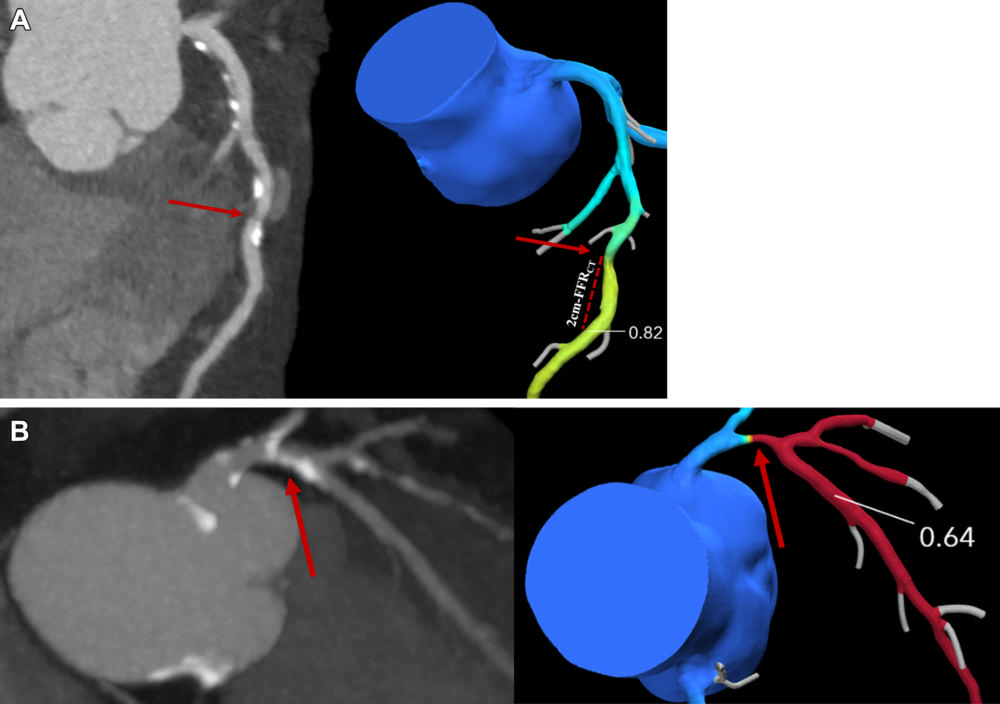
Figure 2. Coronary CT angiography (CTA) images (left side, A and B) and corresponding derived fractional flow reserve (FFR) (right side, A and B). The location 2-cm distal to stenosis is manually delineated and the coronary CTA–derived FFR (FFRCT) value is registered. The lowest lesion-specific coronary CTA–derived FFR value is used to categorize participants, with (A) greater than 0.80 representing a normal value and (B) 0.80 or less representing an abnormal value.
High-res (TIF) version
(Right-click and Save As)
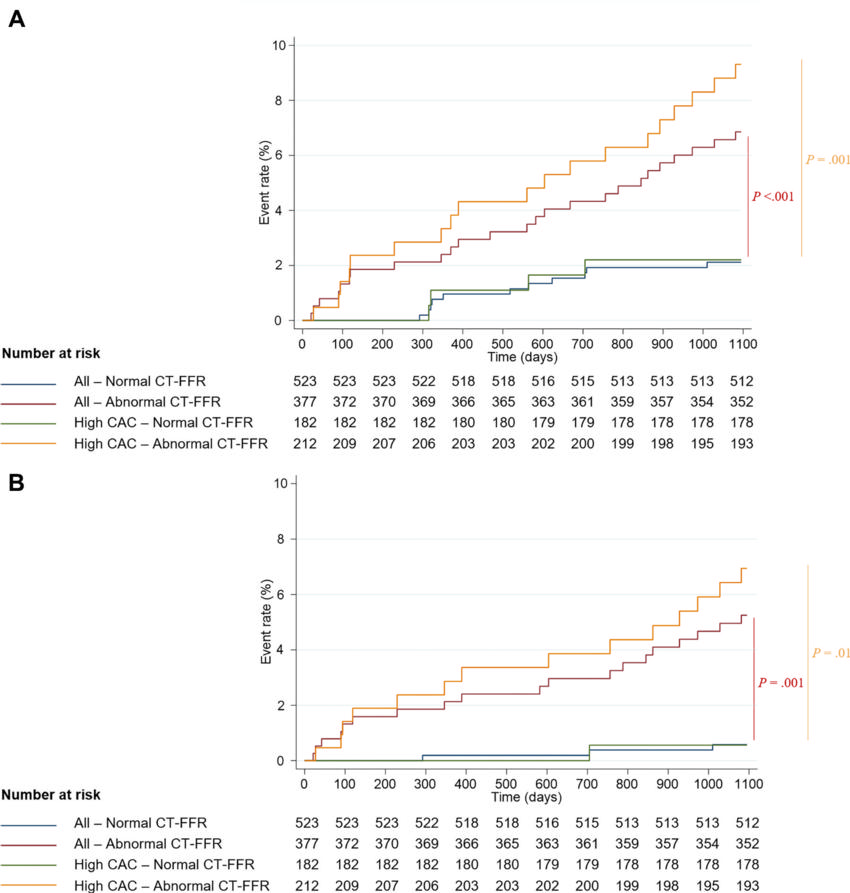
Figure 3. Kaplan-Meier Curves show the primary and secondary study end points in all participants (blue and red lines) and in those with a coronary artery calcium (CAC) score of 400 or greater (green and orange lines), stratified by coronary CT angiography (CTA)–derived fractional flow reserve (FFR; CT-FFR) result. Compared with participants with normal coronary CTA–derived FFR results (value, >0.80), participants with abnormal coronary CTA–derived FFR results (value, ≤0.80) had a higher occurrence of events. This included (A) the primary end point, a composite of all-cause death and spontaneous myocardial infarction (log-rank test P < .001 and P = .001, respectively), and (B) the secondary end point, a composite of cardiovascular death and spontaneous myocardial infarction (log-rank test P = .001 and P = .01, respectively).
High-res (TIF) version
(Right-click and Save As)
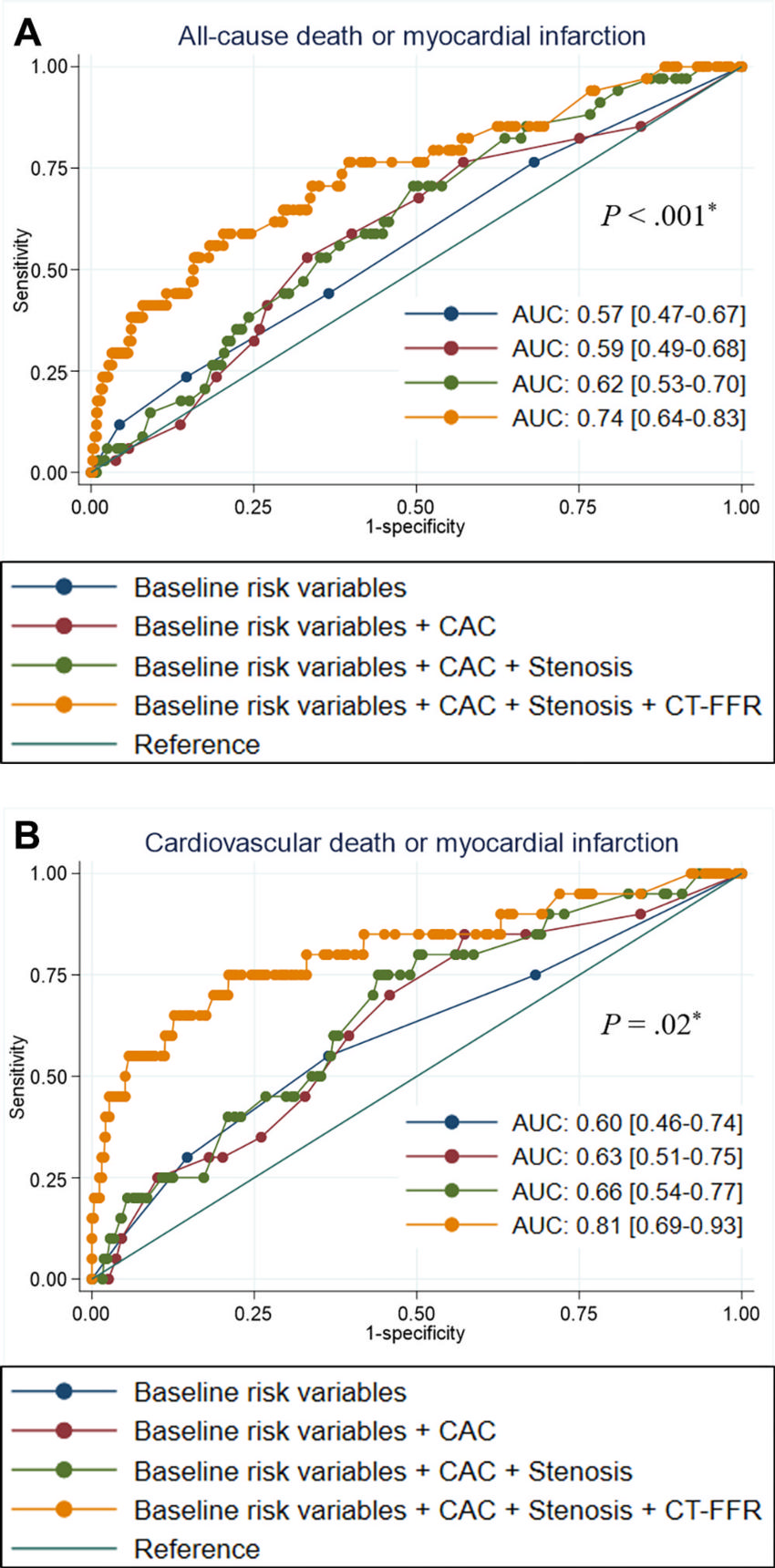
Figure 4. Graphs show performance evaluation of models created using combinations of baseline participant characteristics for discriminating clinical outcomes. Receiver operating characteristic curves show that the model that included baseline risk variables (diabetes, hypertension, dyslipidemia, and ever-smoker), coronary artery calcium (CAC) score categories, coronary stenosis extent category as assessed at coronary CT angiography (CTA), and dichotomous CTA-derived fractional flow reserve (FFR; CT-FFR) results (normal, >0.80; abnormal, ≤0.80) performed best for discriminating (A) primary end point events (area under the receiver operating characteristic curve [AUC], 0.74; DeLong P < .001) and (B) secondary end point events (AUC, 0.81; method by DeLong P < .02). * P values represent the difference between the AUC for baseline risk variables, CAC, and stenosis versus baseline risk variables, CAC, stenosis, and CT-derived FFR.
High-res (TIF) version
(Right-click and Save As)