Photon-Counting CT Offers Superior Imaging in Babies with Heart Defects
Released: May 23, 2023
At A Glance
- Photon-counting computed tomography (PCCT) offers better cardiovascular imaging quality at a similar radiation dose, compared to dual-source CT (DSCT) in infants with suspected cardiac heart defects.
- More than 97% of the PCCT images were at least diagnostic quality, compared to 77% of the DSCT images.
- Congenital heart defects are the leading cause of morbidity and mortality in the neonatal period.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Imani Harris
1-630-481-1009
iharris@rsna.org
OAK BROOK, Ill. — A new advanced form of CT imaging called photon-counting computed tomography (PCCT) offers better cardiovascular imaging quality at a similar radiation dose compared to dual-source CT (DSCT) in infants with suspected cardiac heart defects, according to a study published in Radiology, a journal of the Radiological Society of North America (RSNA).

Congenital heart defects are the leading cause of morbidity and mortality in the neonatal period, occurring in up to one percent of live births. Of those, approximately 25% are critical defects requiring surgical intervention within the first month after birth. A comprehensive assessment, including ultrasound, MRI and CT exams, is typically needed to plan for surgery and to create virtual and printed 3D reconstructions of the heart.
“Infants and neonates with suspected congenital heart defects are a technically challenging group of patients for any imaging method, including CT,” said Timm Dirrichs, M.D., senior physician and specialist in cardiothoracic radiology in the Department of Diagnostic and Interventional Radiology at RWTH Aachen University Hospital in Aachen, Germany. “There is a substantial clinical need to improve cardiac CT of this vulnerable group. It’s essential to carefully map the individual cardiac anatomy and possible routes of surgical intervention using the highest possible diagnostic standards.”
PCCT is an emerging imaging technique that counts the exact number and measures the energy of incoming x-ray photons. Compared with DSCT technology, PCCT offers higher image resolution and/or reduced radiation doses, which is of particular interest when imaging children. The PCCT technique has already been shown to improve cardiovascular CT imaging in adults. However, data on neonates and small children are lacking.
“Our aim was to evaluate the image quality of first-generation photon-counting CT for cardiac imaging in children with suspected cardiac heart defects compared with third-generation dual-source CT (DSCT) and to compare the respective radiation exposure,” Dr. Dirrichs said.
The research team analyzed existing clinical CT exams of 113 children who underwent contrast enhanced PCCT (30 infants), DSCT (83 infants) or both PCCT and DSCT (one infant) of the heart and thoracic aorta between January 2019 and October 2022. The study group consisted of 55 girls/58 boys (median age 66 days).
The researchers found that the PCCT images were sharper, with less image noise and greater contrast than DSCT images. The mean overall visual image quality ratings were higher for PCCT versus DSCT at a similar radiation dose. More than 97% of the PCCT images were at least diagnostic quality, compared to 77% of the DSCT images.
“In our study, none of the PCCT examinations exhibited a poor image quality, and only a few were of limited or moderate quality,” Dr. Dirrichs said.
He noted that of the DSCT images, almost one-quarter were of limited or non-diagnostic quality, and 40% were of moderate quality.
“PCCT is a promising method that may improve diagnostic image quality and efficiency compared to DSCT imaging,” Dr. Dirrichs said. “This higher efficiency can be used to reduce the radiation dose at a given image quality level or to improve image quality at a given radiation level.”
“Photon-counting versus Dual-Source CT of Congenital Heart Defects in Neonates and Infants: Initial Experience.” Collaborating with Dr. Dirrichs were Eric Tietz, M.D., André Rüffer, M.D., Jens Hanten, M.D., Thai Duy Nguyen, M.D., Ebba Dethlefsen, M.D., and Christiane K. Kuhl, M.D.
In 2023, Radiology is celebrating its 100th anniversary with 12 centennial issues, highlighting Radiology’s legacy of publishing exceptional and practical science to improve patient care.
Radiology is edited by Linda Moy, M.D., New York University, New York, N.Y., and owned and published by the Radiological Society of North America, Inc. (https://pubs.rsna.org/journal/radiology)
RSNA is an association of radiologists, radiation oncologists, medical physicists and related scientists promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Illinois. (RSNA.org)
For patient-friendly information on CT and pediatric imaging, visit RadiologyInfo.org.
Images (JPG, TIF):
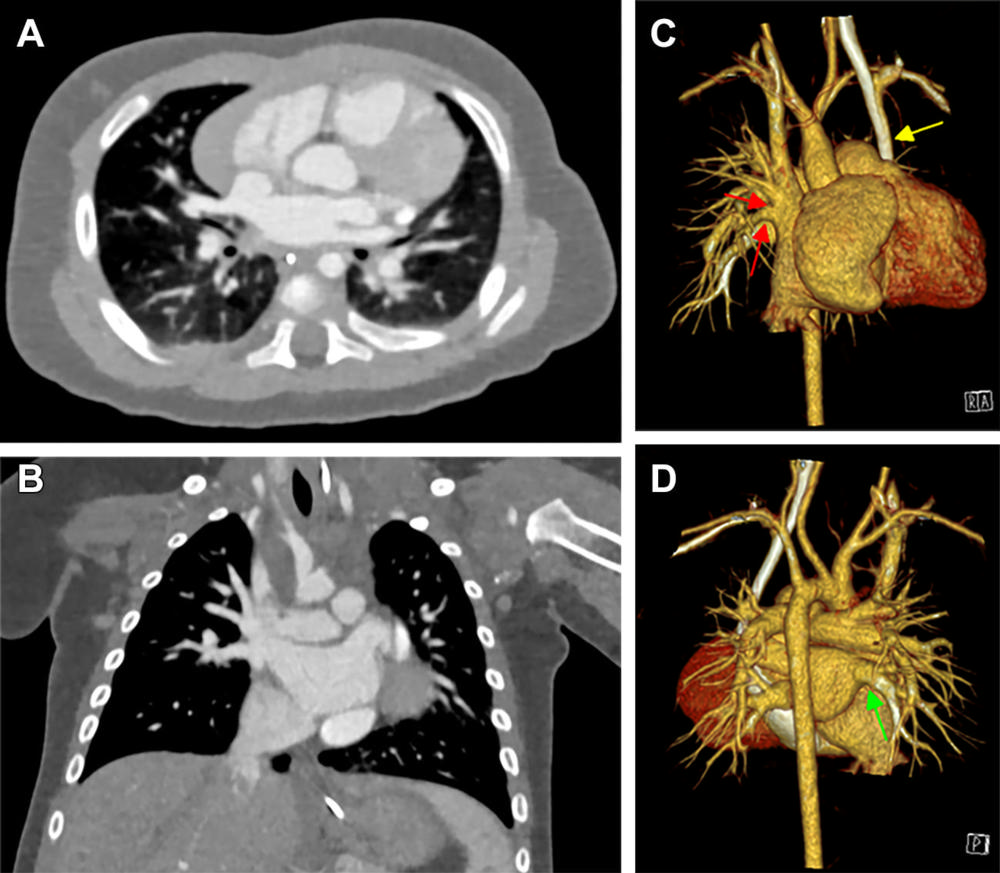
Figure 1. Cardiac photon-counting CT (PCCT) in a 174-day-old male infant with complex congenital heart defect. (A) Contrast-enhanced axial PCCT image shows sonographically suspected sinus venosus defect with partial anomalous pulmonary venous connection. (B) Contrast-enhanced coronal PCCT image. (C) Anterior view of three-dimensional reconstruction shows a partial anomalous pulmonary venous connection of two separate lung veins from the right upper and middle lobe to the right superior vena cava (red arrows) and a persisting left superior vena cava (yellow arrow). (D) Three-dimensional reconstruction, posterior view. The diagnosis was confirmed at PCCT, and PCCT allowed for visualization of the partial anomalous pulmonary venous connection of two separate lung veins from the right upper and middle lobe to the right superior vena cava. One lung vein drains correctly to the left atrium (green arrow). A sinus venosus defect, an atrial septum defect, an enlarged right atrium and a persisting left superior vena cava are shown. The only regular confluence of a single right lung vein into the left atrium is shown (D; green arrow). Image quality was rated as 5 of 5 (optimal).
High-res (TIF) version
(Right-click and Save As)
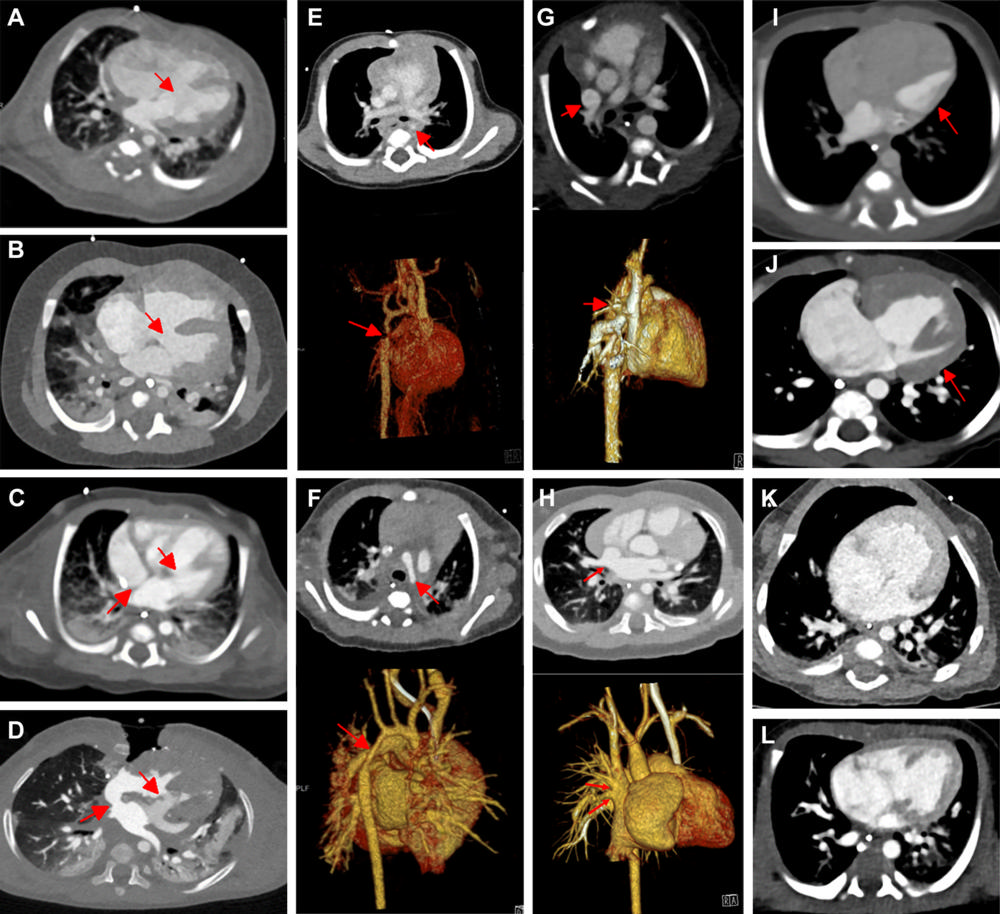
Figure 2. Contrast-enhanced axial dual-source CT (DSCT) versus contrast-enhanced axial photon-counting CT (PCCT) interindividual comparisons in typical congenital heart defects. (A) DSCT image in a 15-day-old male infant suspected at sonography of having ventricular septum defect (arrow). (B) PCCT image in a 155-day-old male infant suspected at sonography of having ventricular septum defect (arrow). (C) DSCT image in a 25-day-old male infant suspected at sonography of having atrioventricular septum defect (arrows). (D) PCCT image in a 355-day-old male infant suspected at sonography of having atrioventricular septum defect (arrows). (E) Contrast-enhanced and three-dimensional (3D) DSCT images in a 128-day-old male infant suspected at sonography of having aortic isthmus stenosis (arrows). (F) Contrast-enhanced and 3D PCCT images in a 16-day-old male infant suspected at sonography of having hypoplastic aortic arch (arrows). (G) Contrast-enhanced and 3D DSCT images in a 63-day-old male infant suspected at sonography of having partial anomalous pulmonary venous connection (arrows). (H) Contrast-enhanced and 3D PCCT images in a 174-day-old male infant suspected at sonography of having partial anomalous pulmonary venous connection (arrows). (I) DSCT image in a 2-day-old male newborn with hypoplastic left heart syndrome (arrow). (J) PCCT image in a 149-day-old male infant with hypoplastic left heart syndrome (arrow). (K) DSCT image in a 10-day-old male newborn with double outlet right ventricle. (L) PCCT image in a 7-day-old female newborn with double outlet right ventricle.
High-res (TIF) version
(Right-click and Save As)
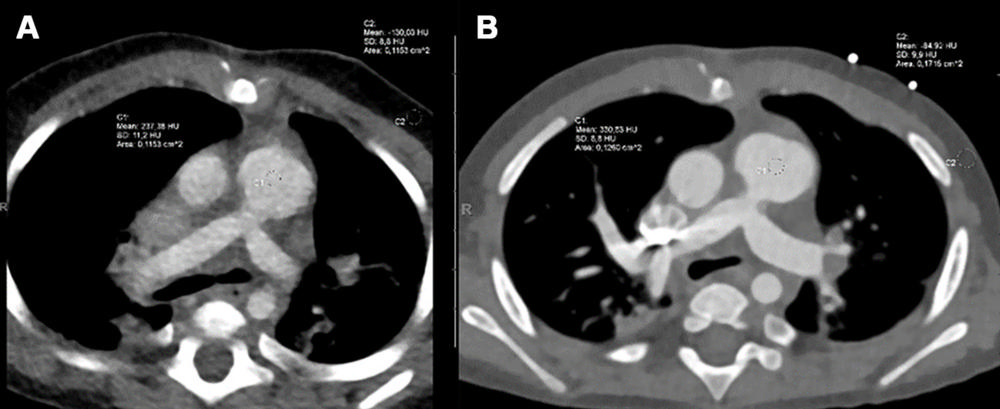
Figure 3. Axial contrast-enhanced dual-source CT (DSCT) and photon-counting CT (PCCT) images for comparison of image quality in the same infant who for clinical reasons underwent both (A) DSCT at 308 days old and (B) PCCT 14 days later at 322 days old. The male infant had a complete ventricular septum defect, Rastelli type A, postoperative situs after stenosis of the left and right lung veins and a so-called sutureless repair, banding of the pulmonary artery, and duct ligation. CT was performed again for clinical reasons (sonographic suspicion of pulmonary venous restenosis). On a five-point scale, the diagnostic image quality score of DSCT (A) was rated as moderate (score of 3), whereas that of PCCT (B) was rated as excellent (score of 5).
High-res (TIF) version
(Right-click and Save As)
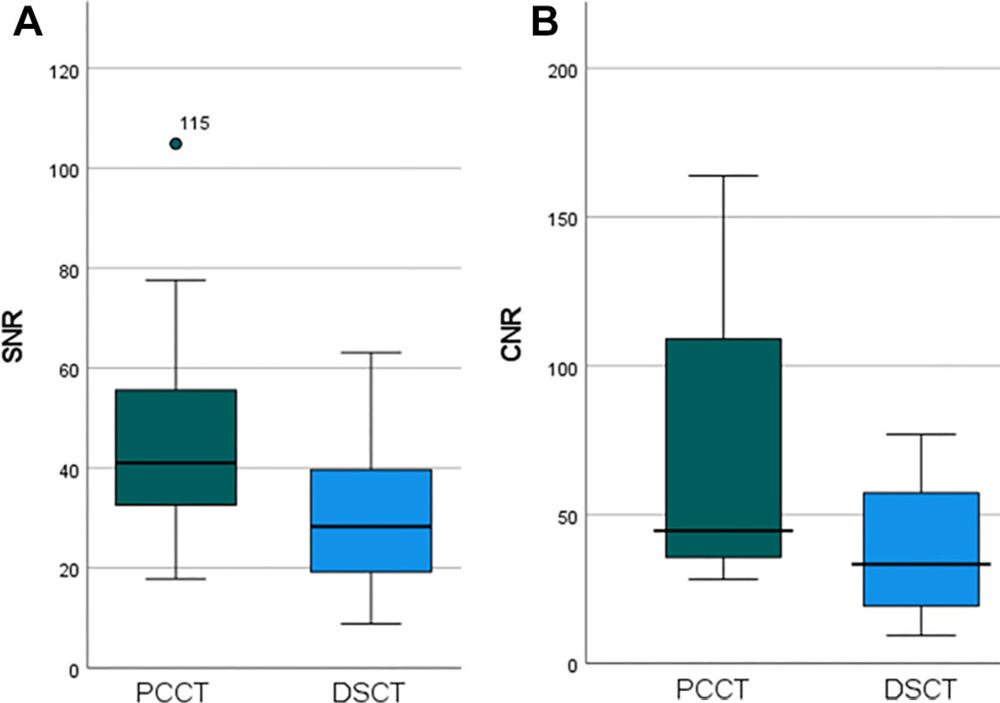
Figure 4. Box and whisker plot shows quantitative assessment of signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR). (A) Mean SNR values of photon-counting CT versus dual-source CT (DSCT) are measured in 4-mm sections. (B) Mean CNR values of PCCT versus DSCT are measured in 4-mm sections. The middle bars in the boxes indicate the median; the whiskers are the lower and upper quartiles. The data point in A is a statistical outlier.
High-res (TIF) version
(Right-click and Save As)
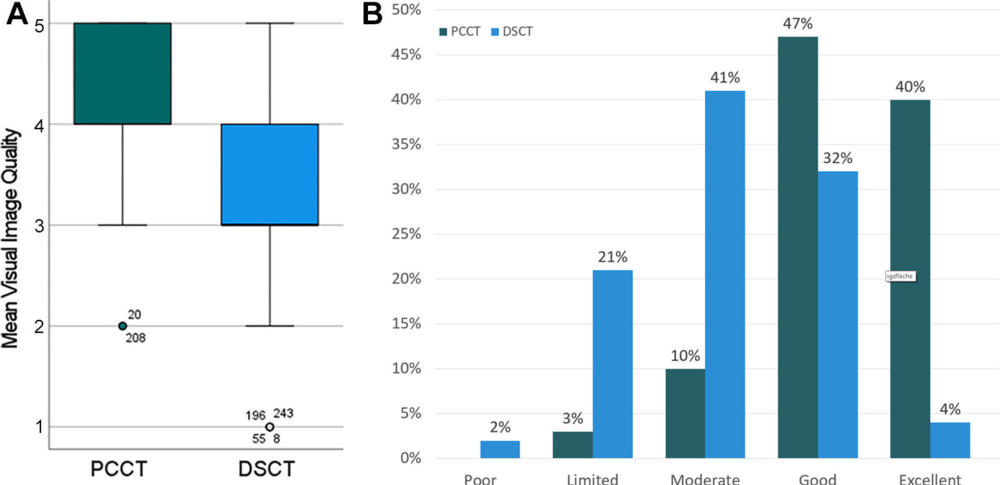
Figure 5. Visual rating of image quality. (A) Mean image quality ratings for PCCT and DSCT on a five-point scale. (B) Distribution of mean image quality ratings between the five-point categories. Points are statistical outliers; whiskers are lower and upper quartiles.
High-res (TIF) version
(Right-click and Save As)