Muscle Fat Linked to Higher Mortality Risk
Released: May 16, 2023
At A Glance
- Asymptomatic adults with a high accumulation of fat in their muscles are at an increased risk of major adverse events and death.
- Myosteatosis was found in 55% of study participants who died.
- The mortality risk of asymptomatic adults with myosteatosis was comparable to the mortality risk associated with smoking or having type 2 diabetes.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Imani Harris
1-630-481-1009
iharris@rsna.org
OAK BROOK, Ill. — Asymptomatic adults with a high accumulation of fat in their muscles, known as myosteatosis, are at an increased risk of major adverse events and death, according to a study published in Radiology, a journal of the Radiological Society of North America (RSNA).

One of the methods used by physicians to estimate body fat in patients is the body mass index (BMI). Since BMI is calculated using only a patient’s height and weight, it’s not an accurate reflection of body composition because patients with similar BMIs can have vastly different co-comorbidities and levels of health risk.
A more thorough reflection of body composition can be obtained from abdominal CT or MRI scans, which can reveal a variety of different fat accumulations. The medical community primarily focuses on visceral fat, which is fat that accumulates around abdominal organs, and liver steatosis, which is a high amount of fat in the liver.
Another form of fat accumulation is myosteatosis, which occurs when fat accumulates in the muscles. Since myosteatosis is usually found in patients who are already sick and undergoing medical imaging for another illness, little is known about its health risks in asymptomatic patients.
“To date, medical imaging with CT or MRI remains the gold standard to evaluate myosteatosis,” said study co-author Maxime Nachit, M.D., Ph.D., a post-doctoral researcher at the Institut de Recherche Expérimentale et Clinique at UCLouvain in Brussels, Belgium.
For this reason, Dr. Nachit and colleagues sought to identify the association between myosteatosis and mortality risk, while simultaneously studying visceral fat, liver steatosis, myopenia (muscle wasting) and obesity.
In the retrospective study, the researchers used an AI tool to extract body composition metrics from abdominal CT scans on asymptomatic adults who had undergone a routine screening for colorectal cancer between 2004 and 2016. Incidences of major adverse events (such as heart attack, stroke, or aneurysm) and death were recorded during an average follow-up period of 8.8 years.
Of the 8,982 adults included in the study, a total of 507 died during the follow-up period. Myosteatosis was associated with an increased risk of major adverse events and was found in 55% of the study participants who died. The absolute mortality risk at 10 years in individuals with myosteatosis was 15.5% compared to obesity (7.6%), liver steatosis (8.5%) or myopenia (9.7%).
While the presence of other health factors, such as visceral fat and liver steatosis, were also associated with a higher mortality risk, myosteatosis remained the highest.
“Interestingly, the relationship was independent from age or markers of obesity such as BMI,” Dr. Nachit said. “In other words, this means that fat accumulation in the muscles is not merely explained by being older and/or having fat overload in other locations of the body.”
The mortality risk of patients with myosteatosis was comparable to the mortality risk associated with smoking or having type 2 diabetes. Despite the growing evidence of the risk factors that are associated with myosteatosis, it is a condition that is still overlooked in the medical community.
Future studies could help determine whether myosteatosis is solely a biomarker of poorer health status or whether it is causally associated with an increased risk of death, according to Dr. Nachit.
“We are witnessing the onset of ‘personalized medicine,’ whose aim is to tailor medical management at the individual level based on a constellation of information such as genetics, medical history, physical characteristics, complex and large-scale molecular evaluation, etc.,” Dr. Nachit said. “Here, we show that myosteatosis – a parameter retrievable from medical images performed routinely in hospitals – is a robust indicator of an individual’s mortality risk at a relatively short term.”
The study was conducted in collaboration with the University of Wisconsin-Madison, where patients were enrolled and scanned under the leadership of co-author Perry J. Pickhardt, M.D. The AI software used in the study was developed in the laboratory of co-author Ronald M. Summers, M.D., Ph.D., at the National Institutes of Health Clinical Center.
“AI-based CT Body Composition Identifies Myosteatosis as Key Mortality Predictor in Asymptomatic Adults.” Collaborating with Dr. Nachit, Pickhardt and Summers were Yves Horsmans, M.D., Ph.D., and Isabelle A. Leclercq, M.D., Ph.D.
In 2023, Radiology is celebrating its 100th anniversary with 12 centennial issues, highlighting Radiology’s legacy of publishing exceptional and practical science to improve patient care.
Radiology is edited by Linda Moy, M.D., New York University, New York, N.Y., and owned and published by the Radiological Society of North America, Inc. (https://pubs.rsna.org/journal/radiology)
RSNA is an association of radiologists, radiation oncologists, medical physicists and related scientists promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Illinois. (RSNA.org)
For patient-friendly information on abdominal CT, visit RadiologyInfo.org.
Images (JPG, TIF):
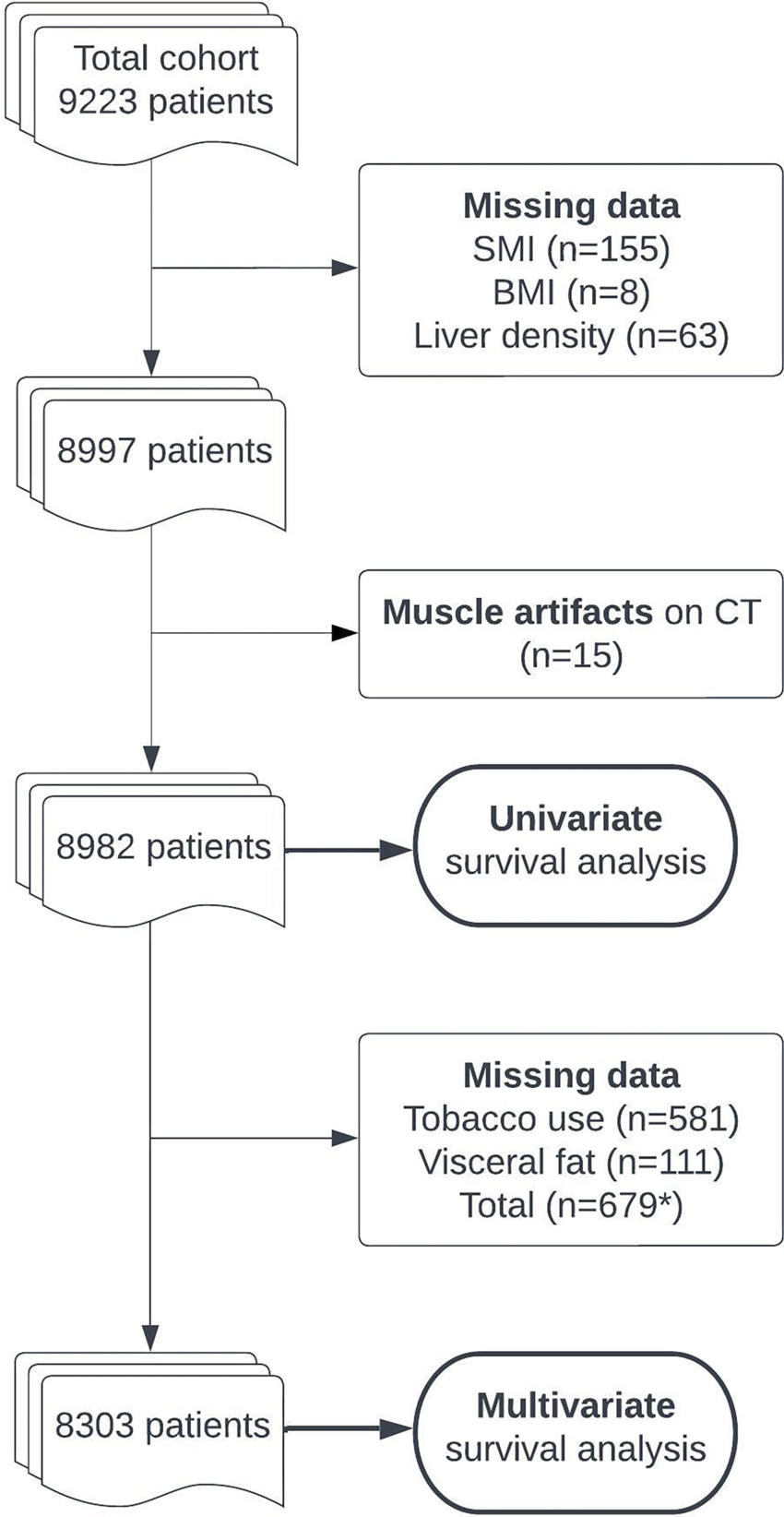
Figure 1. Flowchart shows patient inclusion and exclusion. Patients with missing body composition data (body mass index [BMI], liver density, skeletal muscle index [SMI], or muscle density) or with evident muscle artifacts at CT were excluded before the univariable analysis. Multivariable analysis was performed on the cohort with complete data available, including smoking status, medical history of cardiovascular events, and visceral fat measurements. (* = data were missing in 679 patients, when accounting for overlaps.)
High-res (TIF) version
(Right-click and Save As)
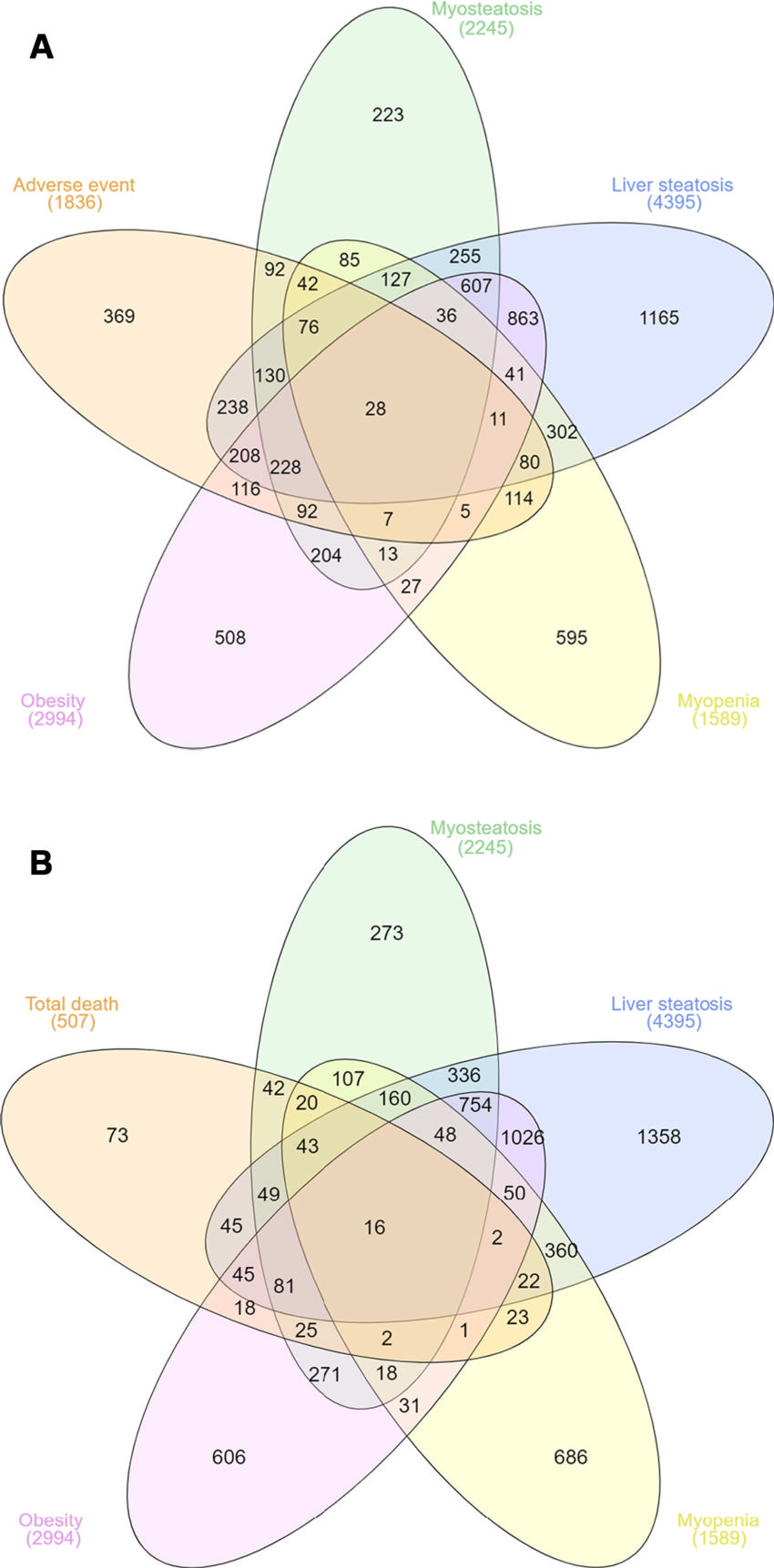
Figure 2. Venn diagrams show the number of patients according to abnormal body composition feature (myosteatosis, liver steatosis, myopenia, obesity) at baseline and their intersection with the number of patients (A) who experienced at least one adverse event (ie, cardiovascular event or death; n = 1836) and (B) who died during follow-up (n = 507). Adverse events mostly occurred in patients with abnormal body composition.
High-res (TIF) version
(Right-click and Save As)
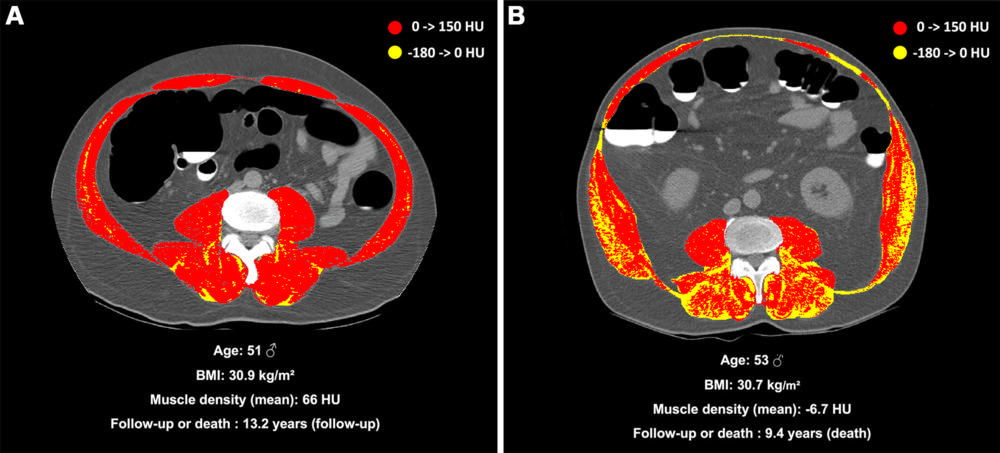
Figure 3. (A) Unenhanced axial abdominal CT image with a Hounsfield unit–based color scale of skeletal muscles in a 51-year-old man with obesity, smoking history, no type 2 diabetes, and no history of cardiovascular events at inclusion shows mild fatty infiltration in the muscles (myosteatosis, yellow), with most voxels in the positive range of Hounsfield units (red). The patient was lost to follow-up after 13.2 years. (B) Unenhanced axial abdominal CT image with a Hounsfield unit–based color scale of skeletal muscles in a 53-year-old man with obesity, smoking history, no type 2 diabetes, and no history of cardiovascular events at inclusion shows severe fatty infiltration in the muscles (myosteatosis, yellow), mostly distributed in the paravertebral (ie, erector spinae and multifidus) and oblique muscle groups. The patient died after 9.4 years of follow-up. BMI = body mass index.
High-res (TIF) version
(Right-click and Save As)
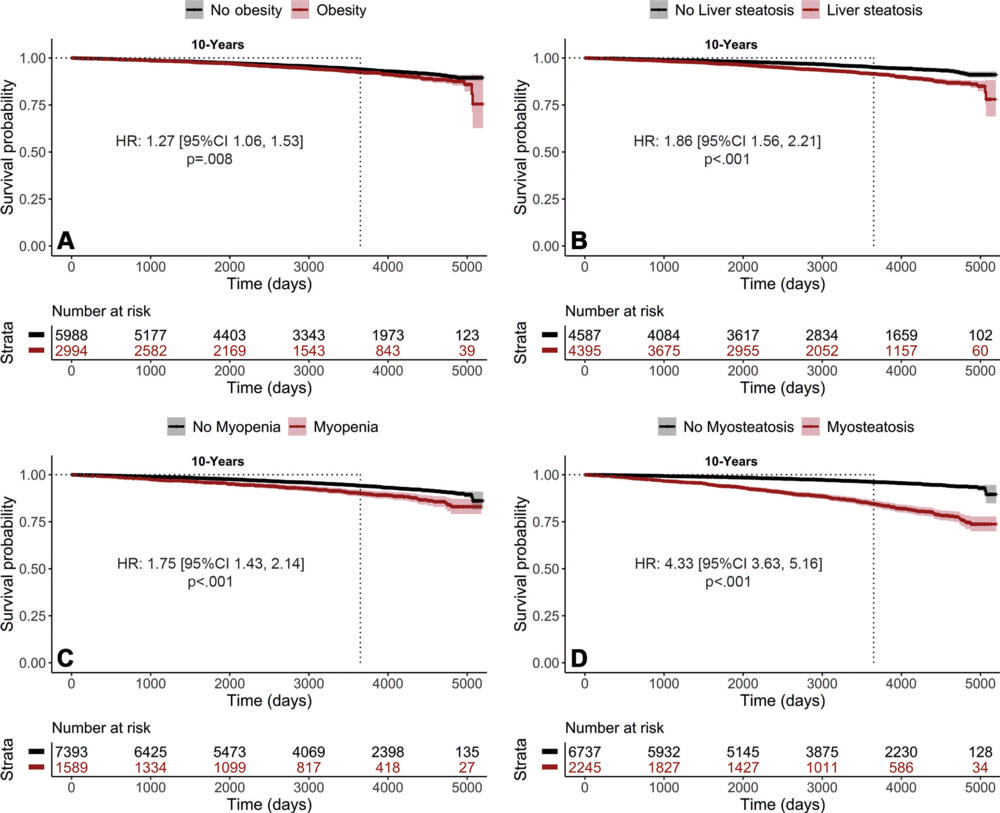
Figure 4. Kaplan-Meier curves of survival probability according to body composition parameter, including (A) obesity, (B) liver steatosis, (C) myopenia, and (D) myosteatosis, show an association between myosteatosis and high mortality risk. Statistics were computed with the Mantel-Cox log-rank test. HR = hazard ratio.
High-res (TIF) version
(Right-click and Save As)
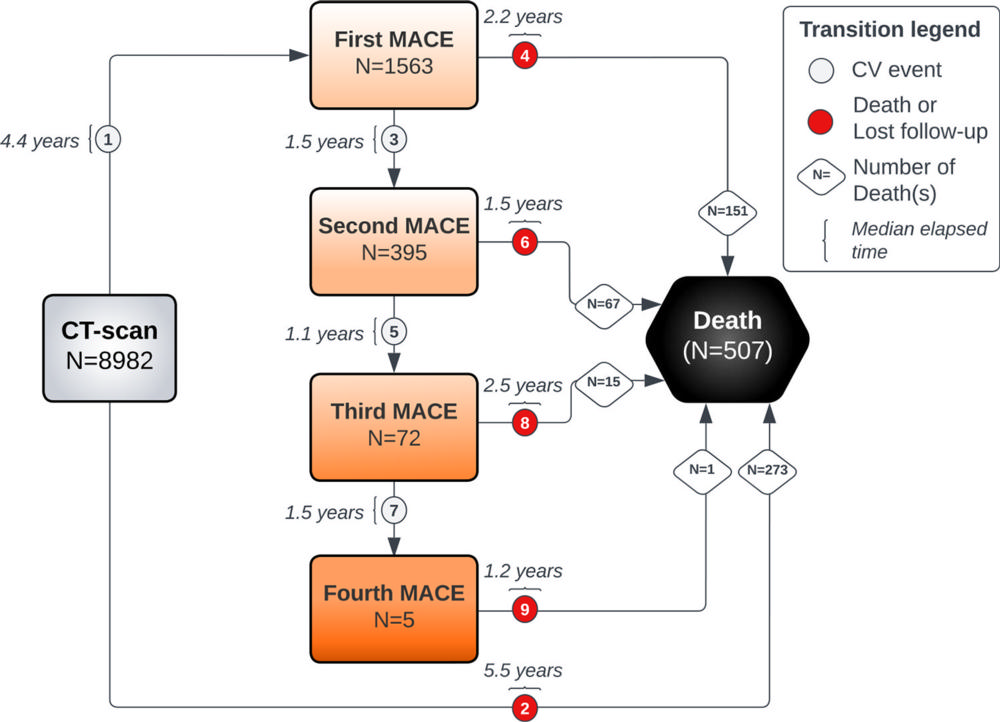
Figure 5. Schematic shows possible transition states of the multistate Markov model, starting at inclusion (ie, CT scan acquisition) and leading to intermediate states (ie, major adverse cardiovascular events [MACEs], indicated by gray circles) and/or to an absorbing state (ie, death or loss to follow-up, indicated by red circles). Transitions numbered 2, 4, 6, 8, or 9 lead to an absorbing state and transitions numbered 1, 3, 5, or 7 lead to an intermediate state. CV = cardiovascular.
High-res (TIF) version
(Right-click and Save As)
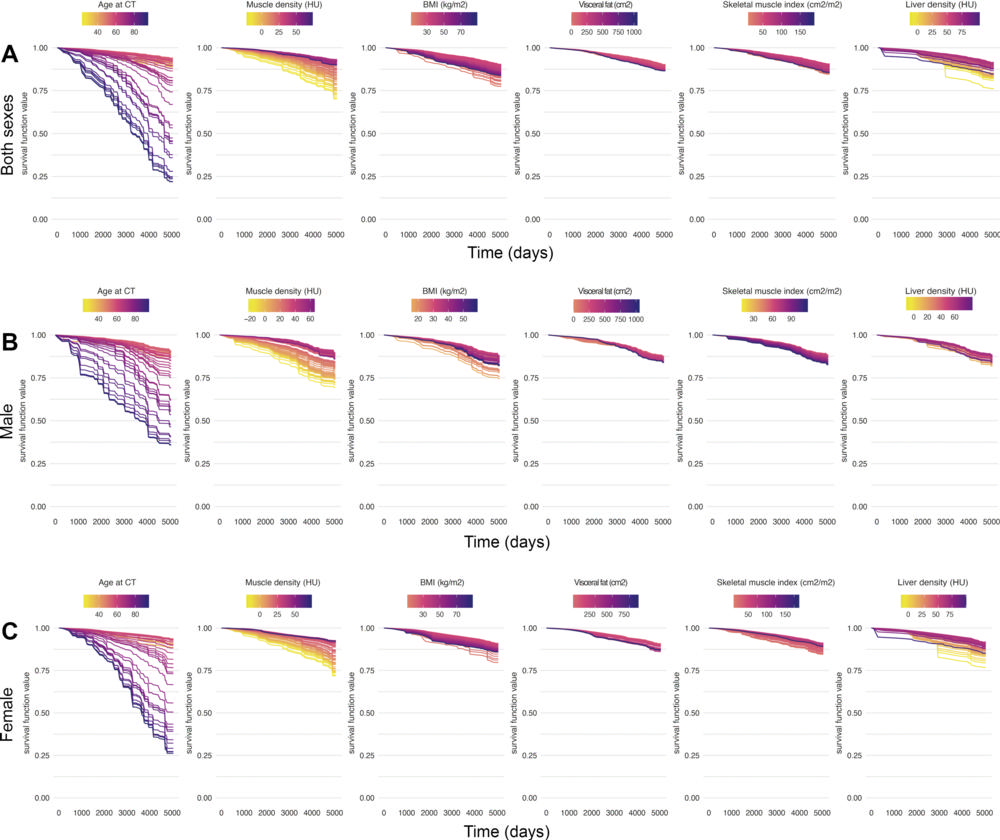
Figure 6. Partial dependence curves extracted from the random forest survival model show the survival function value of each body composition parameter according to (A) sex as a covariate and (B) male and (C) female sex. These results highlight the importance of muscle density in modulating mortality risk (see Appendix S1), independent from the quartile-based stratification; thus, myosteatosis is the most impactful body composition predictor of mortality. BMI = body mass index, HU = Hounsfield unit.
High-res (TIF) version
(Right-click and Save As)