CT Contrast Reaction Raises MRI Contrast Risk
Released: February 22, 2022
At A Glance
- Researchers analyzed more than 330,000 cases of gadolinium-based contrast agent exposure in 154,539 patients over an eight-year period.
- People with a history of allergic-like reactions to iodinated contrast media are susceptible to similar reactions from commonly used MRI contrast agents.
- Premedication or switching to a different MRI contrast agent reduced the risk of reaction.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Imani Harris
1-630-481-1009
iharris@rsna.org
OAK BROOK, Ill. — People with a history of allergic-like reactions to iodinated contrast media, which is used in a variety of X-ray-based procedures, such as CT and angiography, are susceptible to similar reactions from commonly used MRI contrast agents, according to a large, eight-year study published in the journal Radiology. The study also found that premedication or switching to a different MRI contrast agent may reduce risk in patients who have had previous contrast agent reactions.

Gadolinium-based contrast agents (GBCA) have long been used to improve visualization of organs, tissues and blood vessels on MRI and provide a more accurate depiction of disease. Although GBCA are relatively safe, recent studies have reported several adverse reactions related to their use, including allergic-like hypersensitivity reactions, such as rash and flushing.
The incidence of these reactions is increasing with the widespread use of GBCA, prompting an urgent need for research into risk factors, according to the study’s senior author Hye-Ryun Kang, M.D., Ph.D., from the Department of Internal Medicine at Seoul National University College of Medicine in Seoul, Korea.
Dr. Kang and colleagues recently analyzed more than 330,000 cases of GBCA exposure in 154,539 patients over an eight-year period at the Seoul National University Hospital. There were 1,304 cases of allergic-like hypersensitivity reactions, for a rate of 0.4%. In patients who had a previous GBCE reaction, the average recurrence rate was 15%.
Acute allergic-like hypersensitivity reactions, or those that occur within one hour of contrast administration, accounted for 1,178 cases, while a far smaller number of 126 cases were delayed allergic-like hypersensitivity reactions, or those that occur beyond the first hour and mostly within one week after exposure.
The risk of allergic-like hypersensitivity reactions to GBCAs was higher in those with a history of similar reactions to iodinated contrast media. Traditionally, a history of iodinated contrast media hypersensitivity was not considered as a risk factor for hypersensitivity to GBCAs and vice versa, owing to the structural and compositional differences between the two.
“The results of our study challenge this idea,” Dr. Kang said.
The increased risk may be the result of an underlying predisposition to drug allergies in susceptible patients, Dr. Kang said, rather than any cross-reactivity associated with structural similarities between iodinated contrast media and GBCA. In fact, the risk of hypersensitivity reactions to iodinated contrast media was also higher in those who previously experienced a similar reaction to GBCA.
“Thus, physicians should be aware that patients with a history of hypersensitivity to one of iodinated contrast media or GBCA are at greater risk of developing hypersensitivity reactions to the other,” she said.
Analysis of the data showed that premedication, typically with steroids and antihistamines, and changing the GBCA showed preventive effects in patients with a history of acute allergic-like hypersensitivity reactions. Patients who received premedication and before MRI or were switched to a different GBCA showed the lowest rate of recurrence. Only premedication significantly reduced the incidence of reactions in patients with a history of delayed reactions.
“As the most important preventive measure is avoidance of the culprit agent, a precise record of previously used GBCA should be kept for all patients,” Dr. Kang said. “Physicians should discuss appropriate premedication strategies with their patients prior to MRI procedures.”
Dr. Kang emphasized that contrast-enhanced MRI examinations are invaluable in the diagnosis and follow-up of various diseases, and the overall risk remains low.
“As most of these reactions are mild, we believe the benefits of MRI outweigh the potential risks associated with GBCA use,” she said.
Dr. Kang advises that in all patients receiving an MRI with GBCA exposure, a detailed history of previous hypersensitivity allergic reactions be conducted, and when necessary, appropriate prevention measures such as using premedication and switching to different types of GBCA should be implemented.
The researchers hope to conduct future studies with larger populations to identify possible risk factors and effective preventive strategies for delayed hypersensitivity reactions to GBCA.
“Allergic-like Hypersensitivity Reactions to Gadolinium-based Contrast Agents: An 8-Year Cohort Study of 154539 Patients.” Collaborating with Dr. Kang were Yoon Hae Ahn, M.D., Dong Yoon Kang, M.D., Ph.D., Soo-Been Park, B.Pharm., Hyun Hwa Kim, B.Pharm., Hyun Jee Kim, M.S., Ga-Yoon Park, M.D., Soon-Ho Yoon, M.D., Ph.D., Young-Hun Choi, M.D., Ph.D., and Suh Young Lee, M.D., Ph.D.
Radiology is edited by David A. Bluemke, M.D., Ph.D., University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin, and owned and published by the Radiological Society of North America, Inc. (https://pubs.rsna.org/journal/radiology)
RSNA is an association of radiologists, radiation oncologists, medical physicists and related scientists promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Illinois. (RSNA.org)
For patient-friendly information on MRI, CT and contrast materials, visit RadiologyInfo.org.
Images (JPG, TIF):
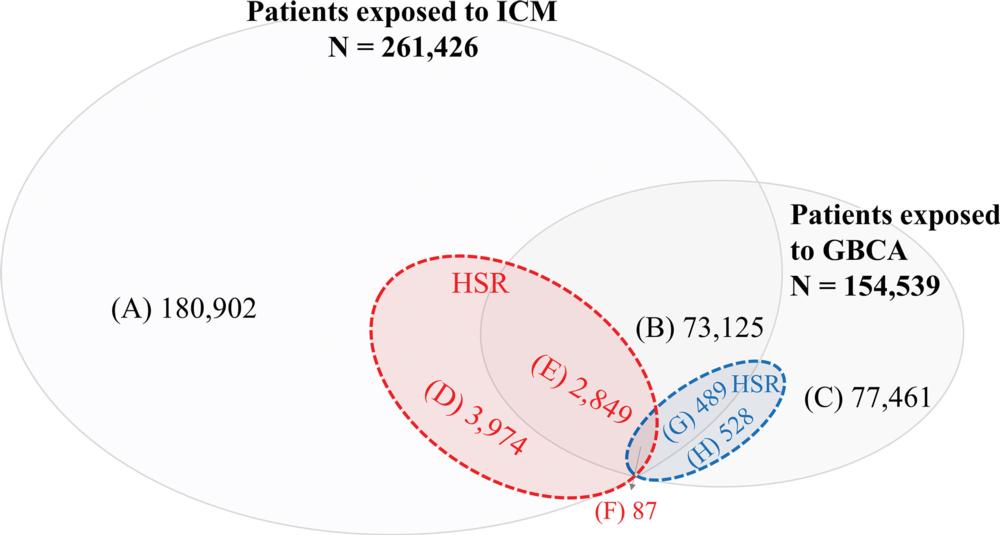
Figure 1. Venn diagram shows hypersensitivity reactions (HSRs) to gadolinium-based contrast agents (GBCAs) and iodinated contrast media (ICM). (A) Number of patients exposed to ICM without HSRs. (B) Number of patients exposed to both ICM and GBCA without HSRs. (C) Number of patients exposed to GBCA without HSRs. (D) Number of patients exposed not to GBCA but to ICM with HSRs. (E) Number of patients exposed to both ICM and GBCA with HSRs to ICM only. (F) Number of patients exposed to both ICM and GBCA with HSRs to both ICM and GBCA. (G) Number of patients exposed to both ICM and GBCA with HSRs to GBCA only. (H) Number of patients exposed not to ICM but to GBCA with HSRs.
High-res (TIF) version
(Right-click and Save As)