Imaging Reveals Bowel Abnormalities in Patients with COVID-19
Released: May 11, 2020
At A Glance
- The study reports findings of bowel abnormalities in patients with COVID-19.
- Bowel findings included wall thickening and findings of ischemia such as pneumatosis (gas in the bowel wall) and portal venous gas.
- Pathology in patients who had bowel resection suggested that ischemia might have been caused by small vessel thrombosis.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Dionna Arnold
1-630-590-7791
darnold@rsna.org
OAK BROOK, Ill. (May 11, 2020) – Patients with COVID-19 can have bowel abnormalities, including ischemia, according to a new study published today in the journal Radiology.
Several studies have evaluated the chest imaging findings in COVID-19, which helped improve understanding of how the disease affects the lungs. More recently, reports have documented that gastrointestinal symptoms, liver injury, and vascular findings are common in these patients. However, abdominal imaging findings have not yet been widely reported. Imaging findings may help physicians understand abdominal manifestations in patients with the infection. Therefore, the authors of this study set out to explore abdominal imaging findings in patients with COVID-19.
The retrospective study included 412 patients consecutively admitted to a single quaternary care center from March 27 to April 10, 2020, who tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The cohort included 241 men (58.5%) and 171 women (41.5%), with an average age of 57 years.

{kind=link}
Records showed that 17% of patients had cross-sectional abdominal imaging, including 44 ultrasounds, 42 CT scans, and 1 MRI. Bowel abnormalities were seen on 31% of CT scans (3.2% of all patients) and were more frequent in intensive care unit (ICU) patients than other inpatients. Bowel findings included thickening and findings of ischemia such as pneumatosis (gas in the bowel wall) and portal venous gas. Surgical correlation in four patients revealed unusual yellow discoloration of bowel in three of the patients, and bowel infarction (dead bowel) in two patients.
“We found bowel abnormalities on imaging in patients with COVID-19, more commonly in sicker patients who went to the ICU,” said Rajesh Bhayana, M.D., FRCPC, abdominal imaging fellow in the Department of Radiology at Massachusetts General Hospital in Boston.
In two patients who had bowel resection, pathology demonstrated ischemia with patchy necrosis (injury due to reduced arterial flow with patchy areas of cell death). Both had fibrin thrombi (blood clots) in submucosal arterioles (small arteries in the bowel wall), suggesting bowel ischemia in these patients might be caused by these small blood clots. Lung base findings led to a diagnosis of COVID-19 in one patient who presented with abdominal symptoms only. Of right upper quadrant ultrasounds, 87% were performed for liver laboratory findings, and 54% demonstrated a dilated sludge-filled gallbladder suggestive of cholestasis, or a decrease in bile flow.
“Some findings were typical of bowel ischemia, or dying bowel, and in those who had surgery we saw small vessel clots beside areas of dead bowel,” Dr. Bhayana said. “Patients in the ICU can have bowel ischemia for other reasons, but we know COVID-19 can lead to clotting and small vessel injury, so bowel might also be affected by this.”
According to the researchers, possible explanations for the spectrum of bowel findings in patients with COVID-19 include direct viral infection, small vessel thrombosis, or nonocclusive mesenteric ischemia. “ACE2 expression is most abundant in lung alveolar epithelial cells, enterocytes of the small intestine, and vascular endothelium suggesting that small bowel and vasculature may be susceptible to SARS-CoV-2 infection,” they wrote.
The authors added that further studies are required to clarify the cause of bowel findings in patients with COVID-19 and to determine whether SARS-CoV-2 plays a direct role in bowel or vascular injury.
“Our study is preliminary, and more work is needed to understand the cause of bowel findings in these patients,” Dr. Bhayana said.
“Abdominal Imaging Findings in COVID-19: Preliminary Observations.” Collaborating with Dr. Bhayana were Avik Som, M.D., Ph.D., Matthew D. Li, M.D., Denston E. Carey, B.Sc., Mark A. Anderson, M.D., Michael A. Blake, M.D., Onofrio Catalano, M.D., Michael S. Gee, M.D., Ph.D., Peter F. Hahn, M.D., Ph.D., Mukesh Harisinghani, M.D., Ph.D., Aoife Kilcoyne M.B.B.Ch., B.A.O., Susanna I. Lee, M.D., Ph.D., Amirkasra Mojtahed, M.D., Pari V. Pandharipande, M.D., M.P.H., Theodore T. Pierce, M.D., David A. Rosman, M.D., M.B.A., Sanjay Saini, M.D., Anthony E. Samir, M.D., M.P.H., Joseph F. Simeone, M.D., Debra A. Gervais, M.D., George Velmahos, M.D., Ph.D., Joseph Misdraji, M.D., and Avinash Kambadakone, M.D., FRCR.
Radiology is edited by David A. Bluemke, M.D., Ph.D., University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin, and owned and published by the Radiological Society of North America, Inc. (https://pubs.rsna.org/journal/radiology)
RSNA is an association of radiologists, radiation oncologists, medical physicists and related scientists promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Illinois. (RSNA.org)
For patient-friendly information on abdominal imaging, visit RadiologyInfo.org.

Figure 1. Axial (A) and coronal (B) CT of the abdomen and pelvis with IV contrast in a 57-year-old man with a high clinical suspicion for bowel ischemia. There was generalized small bowel distension and segmental thickening (arrows), with adjacent mesenteric congestion (thin arrow in B), and a small volume of ascites (* in B). Findings are nonspecific but suggestive of early ischemia or infection.
High-res (TIF) version
(Right-click and Save As)

Figure 2. Coronal CT of the abdomen and pelvis with IV contrast in a 47-year-old man with abdominal tenderness demonstrates typical findings of mesenteric ischemia and infarction, including pneumatosis intestinalis (arrow) and non-enhancing bowel (*). Frank discontinuity of a thickened loop of small bowel in the pelvis (thin arrow) is in keeping with perforation.
High-res (TIF) version
(Right-click and Save As)
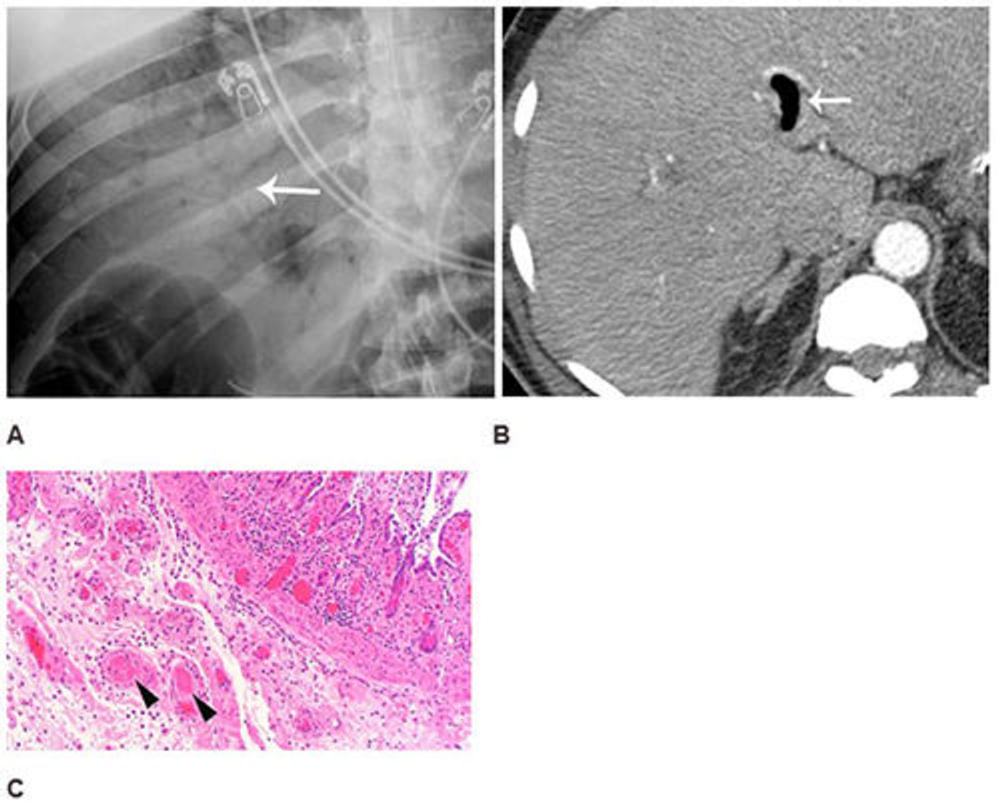
Figure 3. Abdominal radiograph (A) in a 52-year-old man demonstrates portal venous gas (thin arrow in A), suggestive of bowel infarction. Post-operative CT (B) also demonstrates portal venous gas (thin arrow in B). At laparotomy, ischemic and necrotic bowel was identified along with an atypical yellow discoloration of small bowel. Photomicrograph (H and E, 400x) (C) demonstrated submucosal arterioles with fibrin thrombi (arrowheads). The overlying mucosa (upper right) is partially necrotic with crypt dropout and partial loss of the surface epithelium.
High-res (TIF) version
(Right-click and Save As)
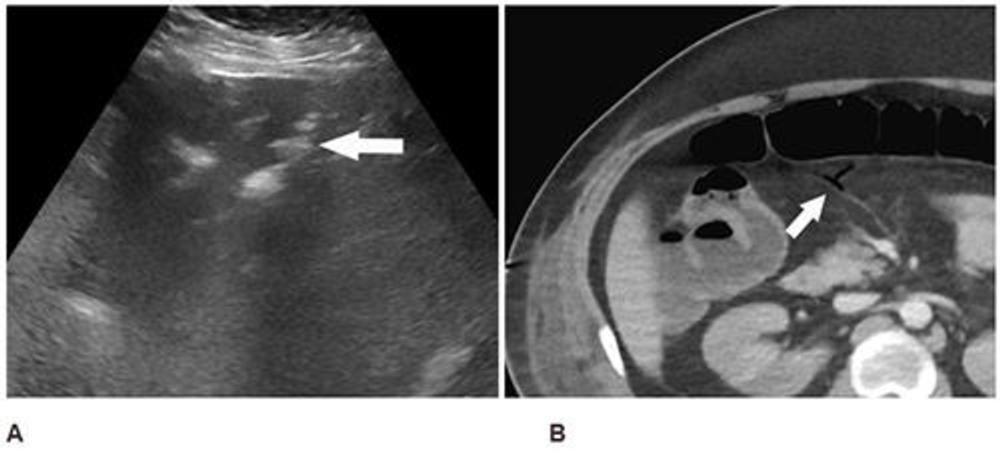
Figure 4. Abdominal ultrasound (A) performed for elevated liver enzymes in a 34-year-old man incidentally noted peripheral echogenic branching foci (arrow) with dirty shadowing (*), in keeping with portal venous gas. Subsequent CT abdomen and pelvis with IV contrast (B) confirmed portal venous gas and demonstrated gas in the transverse mesocolon vasculature (arrow). At laparotomy, patchy areas of yellow discoloration were identified on the antimesenteric aspect of the transverse colon of uncertain etiology. Second look laparotomy demonstrated yellow discoloration of the stomach and no ischemia.
High-res (TIF) version
(Right-click and Save As)
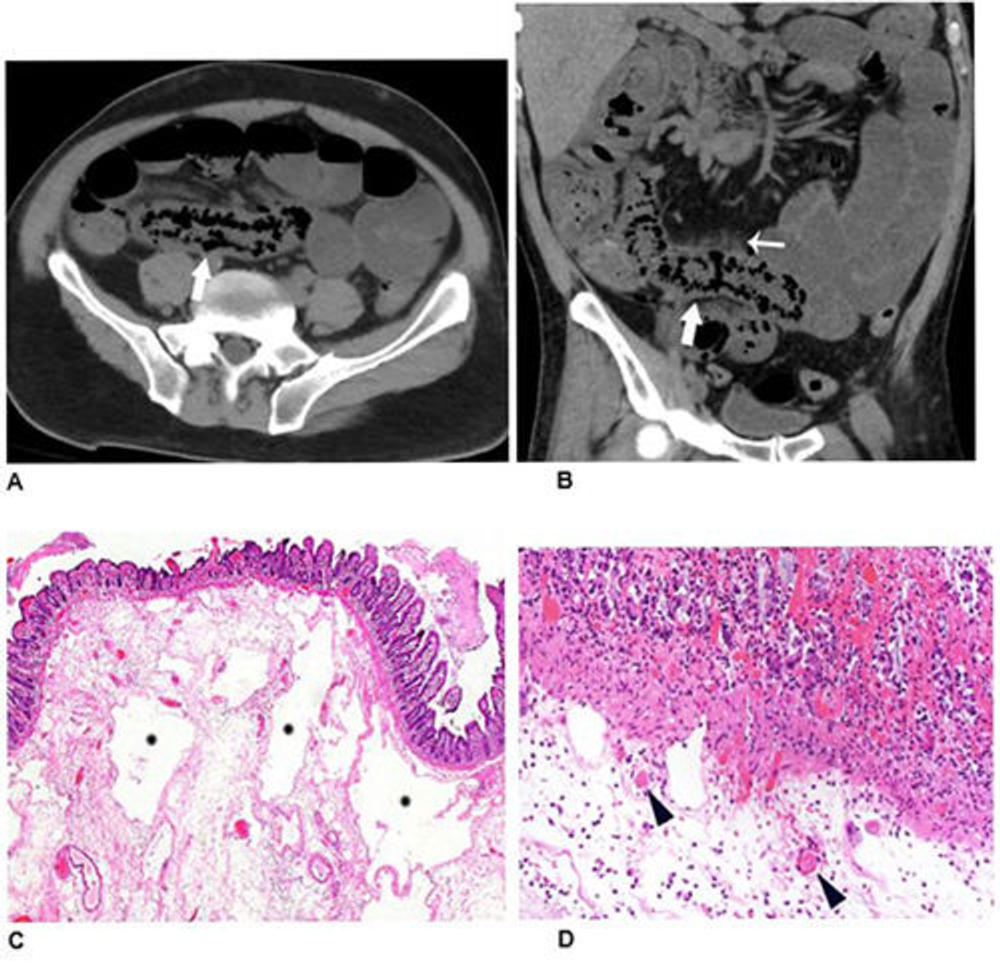
Figure 5. Non-contrast axial (A) and coronal (B) CT performed in a 54-year-old man demonstrates pneumatosis cystoides intestinalis (arrows) in a long segment of ileum. Adjacent mesenteric congestion is also noted (thin arrow). Laparotomy demonstrated no frank bowel necrosis. Low power photomicrograph (H and E, 40x) of the ileum (C) shows ischemic degenerative changes of the mucosa with villous blunting (left) and withered crypts. There is marked submucosal edema with large empty spaces consistent with pneumatosis (*). High power view (H and E, 400x) (D) of the superficial submucosa shows arterioles with fibrin thrombi (arrowheads) beneath the damaged mucosa.
High-res (TIF) version
(Right-click and Save As)