Greater Left Ventricular Mass Increases Risk of Heart Failure
Released: August 27, 2019
At A Glance
- An increase of the heart's left ventricular mass is a strong predictor of cardiovascular-related death.
- Researchers analyzed data from 4,988 study participants over a 15-year period.
- Individuals with left ventricular hypertrophy had 4.3 times the risk of coronary artery disease-related death.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Dionna Arnold
1-630-590-7791
darnold@rsna.org
OAK BROOK, Ill. — Elevated left ventricular mass, known as left-ventricular hypertrophy, is a stronger predictor of coronary artery disease-related death and heart failure than coronary artery calcium score, according to a new study published in the journal Radiology.
In the study led by Nadine Kawel-Boehm, M.D., a senior staff radiologist at Hospital Graubünden in Chur, Switzerland, a team of researchers analyzed data collected in the Multi-Ethnic Study of Atherosclerosis (MESA) sponsored by the National Heart, Lung, and Blood Institute. MESA is an ongoing, multi-center study of a diverse, population-based sample of 6,814 men and women age 45-84 with no known heart disease.
According to Dr. Kawel-Boehm, there is little research on predicting the long-term risk of cardiovascular events in ethnically diverse patients who have MRI-identified left ventricular (LV) hypertrophy, a condition in which the muscle mass of the heart's main pumping chamber is increased.
"Previous studies have used ECG or echocardiography, which have lower sensitivity in the diagnosis of LV hypertrophy, and typically follow patients for only several years," she said. "The MESA study used MRI, which is the gold standard for quantifying LV mass, and had a long follow-up of 15 years."
The researchers studied otherwise healthy individuals from the community in the MESA study. 4,988 MESA participants underwent a baseline cardiac MRI between 2000 and 2002 and participated in follow-up over a 15-year period. MRI showed that 247 participants in the study group had LV hypertrophy.
The mean age of all participants at baseline was 62 years, and 52 percent were women. Thirty-nine percent were white, 13 percent were Asian, 26 percent were African American and 22 percent were Hispanic.
At the 15-year follow-up, the research team found that 290 patients had a significant coronary heart disease (CHD) event, including 207 myocardial infarctions—or heart attacks, and 95 CHD deaths. Cardiovascular disease-related deaths occurred in 57 patients, and 215 patients had heart failure.
A statistical analysis of the data demonstrated that LV hypertrophy was an independent predictor of significant CHD events, including myocardial infarction, coronary artery disease-related death and heart failure.
According to the analysis, 22 percent of the study participants with LV hypertrophy had a significant CHD event, compared to 6 percent of participants without LV hypertrophy.
Patients with LV hypertrophy had 4.3 times the risk of coronary artery disease-related death compared to participants without LV hypertrophy. Deaths from coronary and non-coronary related cardiovascular causes were more strongly related to LV hypertrophy than to coronary artery calcium scoring done with a CT scan.
"In contrast to the widely used coronary artery calcium by CT, which measures a condition not known to regress under medical therapy, an elevated LV mass is potentially reversible under treatment," Dr. Kawel-Boehm said.
As a result of the long length of the study follow-up, Dr. Kawel-Boehm said the researchers were able to determine that the risk of cardiovascular events began to increase in participants with LV hypertrophy particularly after five years.
"Our results provide further evidence and motivation for regular follow up and management of individuals with left ventricular hypertrophy," she said. "A higher LV mass quantified by imaging may matter more in some instances than a high calcium score."
"Left Ventricular Mass at MRI and Long-Term Risk of Cardiovascular Events: The Multi-Ethnic Study of Atherosclerosis (MESA)." Collaborating with Dr. Kawel-Boehm were Richard Kronmal, Ph.D., John Eng, M.D., Aaron Folsom, M.D., Gregory Burke, M.D., J. Jeffrey Carr, M.D., M.Sc., Steven Shea, M.D., M.S., João A. C. Lima, M.D., and David A. Bluemke, M.D., Ph.D.
Radiology is edited by David A. Bluemke, M.D., Ph.D., University of Wisconsin School of Medicine and Public Health, Madison, Wis., and owned and published by the Radiological Society of North America, Inc. (http://radiology.rsna.org/)
RSNA is an association of over 53,400 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on cardiovascular imaging, visit RadiologyInfo.org.
Images (.JPG and .TIF format)
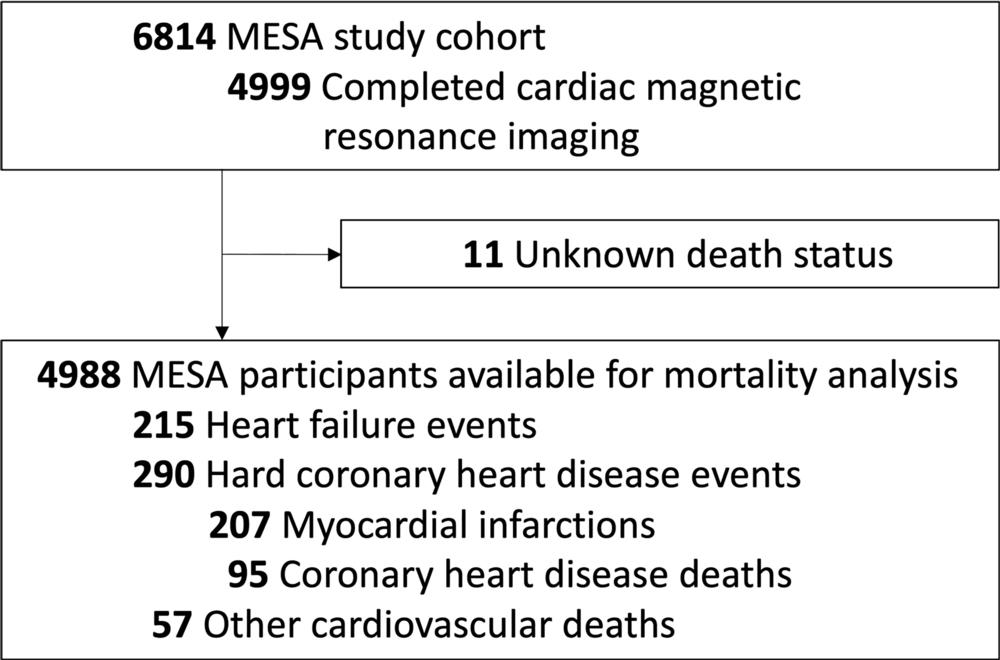
Figure 1. Flow diagram of events. Hard coronary heart disease events were a composite end point and included myocardial infarction and coronary artery disease–related death. The sum of myocardial infarction and coronary artery disease–related deaths does not equal the number of hard coronary heart disease events because some participants had myocardial infarction followed by coronary artery disease–related death. Other cardiovascular death excluded stroke and was adjudicated not to be atherosclerotic in origin (eg, pulmonary embolism, arrhythmia, and cardiomyopathy). MESA = Multi-Ethnic Study of Atherosclerosis.
High-res (TIF) version
(Right-click and Save As)
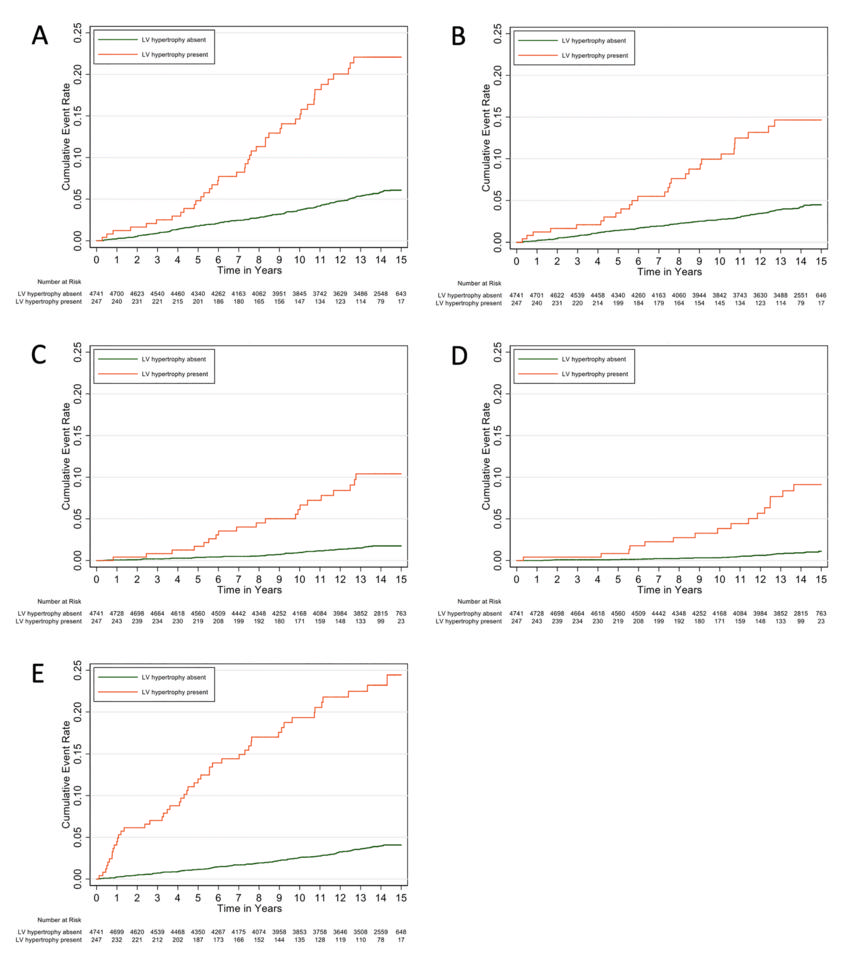
Figure 2. Kaplan-Meier analysis of the cumulative incidence of, A, hard coronary heart disease events, B, myocardial infarction, C, coronary artery disease–related death, D, other cardiovascular death events, and, E, heart failure for participants with left ventricular (LV) hypertrophy versus those without LV hypertrophy.
High-res (TIF) version
(Right-click and Save As)