Researchers Study Surveillance MRI in Breast Cancer Survivors
Released: June 04, 2019
At A Glance
- Annual screening with surveillance mammography is recommended for the millions of breast cancer survivors in the United States.
- Adding MRI to mammography in these annual surveillance exams may detect more cancers but substantially increases benign biopsy rate, according to a study of 13,266 survivors.
- The study also found that the use of breast MRI was associated with younger age at diagnosis and use of chemotherapy, as well as higher education and income.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Dionna Arnold
1-630-590-7791
darnold@rsna.org
OAK BROOK, Ill. — The addition of breast MRI to mammography in screening breast cancer survivors for new cancers results in higher cancer detection rates, but also more biopsies that are benign, according to a large study published in the journal Radiology.

{kind=link}
Annual screening with surveillance mammography is recommended for the millions of breast cancer survivors in the United States. A small but growing proportion of women who had breast cancer receive breast MRI as an adjunct to surveillance mammography, despite a lack of consensus among national clinical organizations over the practice. Evidence is limited on benefits and potential harms of breast MRI for breast cancer survivors.
"People often think more testing is better," said lead author Karen J. Wernli, Ph.D., an associate investigator at the Kaiser Permanente Washington Health Research Institute in Seattle. "That might be true for some women, but not necessarily all. It's important for clinicians and women to be aware of both the benefits and harms that can come from imaging."
In the largest and most comprehensive study of its kind to date, Dr. Wernli and colleagues compared the performance of breast MRI to mammography alone in 13,266 women aged 18 or older years who had survived breast cancer. Collectively, the women had received 34,938 mammograms and 2,506 breast MRI examinations from 2005-2012 to screen for second breast cancers. The data was drawn from five sites in the Breast Cancer Surveillance Consortium: the Carolina Mammography Registry, Kaiser Permanente Washington, the New Hampshire Mammography Network, the San Francisco Mammography Registry and the Vermont Breast Cancer Surveillance System.
Breast MRI had a slightly higher cancer detection rate than mammography alone. To achieve that higher rate, nearly twice as many women had to get breast biopsy, something that has been shown to heighten anxiety in women with prior breast cancer.
The breast MRI cancer detection rate was 10.8 per 1,000 examinations vs. 8.2 for mammography alone. The breast MRI biopsy rate was 10.1 percent. The mammography biopsy rate was 4.0 percent.
There were no significant differences between the two imaging modalities in sensitivity, or the ability to distinguish breast cancer from other findings. Rates of interval cancers, or cancers that emerged between screenings, were similar in the two groups, indicating that mammography did not miss more cancers that would become clinically detectable during the one-year surveillance interval.
In contrast to earlier studies of breast MRI performance, the researchers incorporated individual characteristics of women, such as education and income, into their analysis, along with treatment and primary cancer diagnosis. They found that the use of breast MRI was associated with younger age at diagnosis and use of chemotherapy, as well as higher education and income.
The results underscore the complexity of decisions involving the introduction of new imaging tests into cancer screening programs and support the importance of proceeding with caution, according to Dr. Wernli.
"It's really important for us to know that when we're making guideline recommendations and conclusions that we really look at the best quality of the evidence," she said. "It's also very important to adjust for differences among women when we're trying to evaluate the addition of new imaging tests to surveillance mammography."
"Surveillance Breast MRI and Mammography: Comparison in Women with a Personal History of Breast Cancer." Collaborating with Dr. Wernli were Laura Ichikawa, M.S., Karla Kerlikowske, M.D., Diana S. M. Buist, Ph.D., Susan D. Brandzel, M.P.H., Mary Bush, M.S., Dianne Johnson, B.A., Louise M. Henderson, Ph.D., Larissa Nekhlyudov, M.D., Tracy Onega, Ph.D., Brian L. Sprague, Ph.D., Janie M. Lee, M.D., Constance D. Lehman, M.D., and Diana L. Miglioretti, Ph.D.
Radiology is edited by David A. Bluemke, M.D., Ph.D., University of Wisconsin School of Medicine and Public Health, Madison, Wis., and owned and published by the Radiological Society of North America, Inc. (http://radiology.rsna.org/)
RSNA is an association of over 53,400 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on breast MRI, visit RadiologyInfo.org.
Images (.JPG and .TIF format)
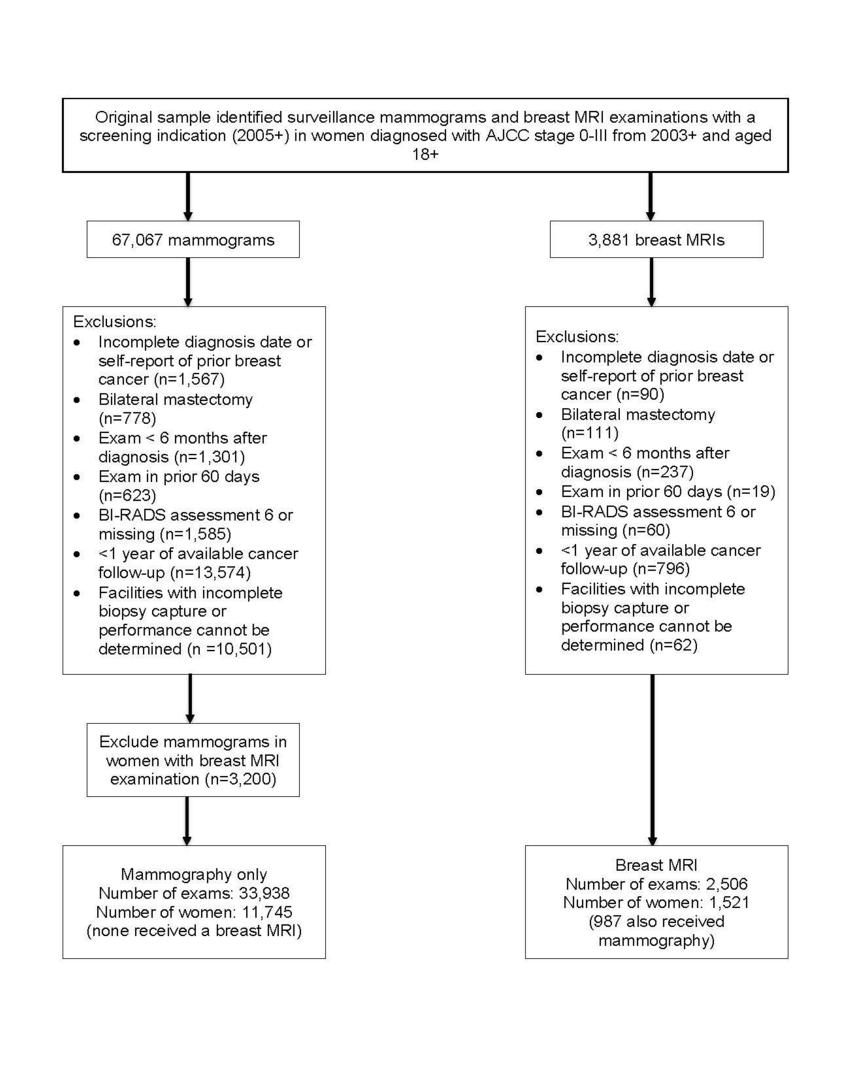
Figure 1. Consort diagram of study flow, Breast Cancer Surveillance Consortium, 2005–2012.
High-res (TIF) version
(Right-click and Save As)