New Report Details Pre- and Postnatal Brain Defects from Zika Virus
Released: August 23, 2016
At A Glance
- Researchers from the epicenter of the current Zika virus outbreak have released a report on imaging findings in babies and fetuses infected with the Zika virus.
- Zika virus is most dangerous when transmitted from a pregnant mother to her fetus, increasing the likelihood of severe brain defects in the baby.
- In addition to microcephaly, the report identifies a wide array of brain defects, visible on CT, MRI and ultrasound.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org
OAK BROOK, Ill. — The journal Radiology has published a special report, detailing the spectrum of imaging findings in babies and fetuses infected with the Zika virus.
"Imaging is essential for identifying the presence and the severity of the structural changes induced by the infection, especially in the central nervous system," said the report's lead author, Fernanda Tovar-Moll, M.D., Ph.D., vice president of the D'Or Institute for Research and Education and professor at the Federal University of Rio de Janeiro, in Rio de Janeiro, Brazil. "Microcephaly is just one of several radiological features."
Zika appears to be most dangerous when transmitted from a pregnant mother to her fetus during the first trimester of pregnancy, increasing the likelihood of severe brain defects in the baby, including microcephaly. In cases of microcephaly, the baby's head is exceptionally small, due to an underdeveloped brain. Zika has also been linked to eye defects, hearing impairment and stunted growth in babies.
"The first trimester is the time where infection seems to be riskiest for the pregnancy," said study coauthor Deborah Levine, M.D., director of Obstetric & Gynecologic Ultrasound at Beth Israel Deaconess Medical Center and professor of radiology at Harvard Medical School in Boston. "From an imaging standpoint, the abnormalities in the brain are very severe when compared to other congenital infections."
Though much of the concern in the media regarding the toxic effects of Zika virus has focused on brain findings of microcephaly, the researchers noted that there are a variety of brain abnormalities that can be found in fetuses exposed to the virus, including gray and white matter volume loss, brainstem abnormalities, calcifications, and a condition called ventriculomegaly, where the ventricles, or fluid filled spaces in the brain, are enlarged. Some babies infected by Zika may not have a small head size if the ventricles remain excessively enlarged.
The researchers performed a retrospective review of imaging and autopsy findings associated with congenital Zika virus infection found in the Instituto de Pesquisa in Campina Grande state Paraiba (IPESQ) in Northeastern Brazil, where the infection has been severe.
From June 2015 to May 2016, 438 patients were referred to the IPESQ due to rash during pregnancy or suspected central nervous system abnormality. From this group, the researchers identified 17 fetuses or neonates of women who had imaging at IPESQ, as well as documented Zika infection in fluid or tissue ("confirmed cohort"), and 28 fetuses or neonates with brain findings suspicious for Zika infection with intracranial calcifications ("presumed cohort"). Imaging exams included fetal MRI, postnatal brain CT, postnatal brain MRI and, in some cases, longitudinal prenatal ultrasound.
The brain abnormalities seen in confirmed and presumed Zika groups were very similar. Nearly all of the babies in each group had ventriculomegaly. Although most fetuses had at least one exam showing abnormally small head circumference, the researchers discovered that head circumference was normal in three fetuses with severe ventriculomegaly.
Ninety-four percent of the confirmed Zika group and 79 percent of the presumed Zika group had abnormalities of the corpus callosum, which is a large nerve fiber bundle that allows communication between the left and right hemispheres of the brain. All but one had cortical migrational abnormalities, meaning the neurons did not travel to their proper destination in the brain.
Intracranial calcifications were present in almost all of the neonates, most commonly found at the gray-white junction of the brain. All of the babies exhibited reduced tissue volume in their brains. All patients showed varying abnormalities in cortical development.
"The severity of the cortical malformation and associated tissue changes, and the localization of the calcifications at the grey-white matter junction were the most surprising findings in our research," Dr. Tovar-Moll said.
The babies' skulls frequently had a collapsed appearance with overlapping sutures and redundant skin folds. The researchers believe the unusual appearance of the skull is due to a combination of the small brain as it develops, but also a result of what at some point was likely a larger head size—due to ventriculomegaly—that then decompresses, and/or brain atrophy, giving the skull the collapsed shape.
Dr. Levine noted that ultrasound in pregnancy can show the abnormalities associated with congenital Zika infection, but it may take time before these changes are obvious.
"More than one ultrasound or MRI scan in pregnancy may be needed to assess the growth and development abnormalities of the brain," she said.
Zika is mainly spread to humans via the bite of an infected mosquito. Symptoms may include fever, rash, joint or muscle pain, headache, and bloodshot eyes. However, many people infected with Zika have no symptoms at all. Although the current Zika outbreak is centered in Brazil, it has spread to countries and territories around the world, including the United States.
Pregnant women and women who are considering becoming pregnant should avoid visiting areas where infected mosquitos are known to be present. However, if women live in areas where the mosquitos are present, the recommendation of the Centers for Disease Control and Prevention (CDC) is to wear clothes that protect from mosquito bites, use mosquito repellent and get appropriate testing, including routine prenatal care and an ultrasound at 18 to 20 weeks. Pregnant women who are worried that they may have contracted the virus should speak with their obstetrician to initiate testing.
Dr. Tovar-Moll noted that the researchers are continuing to investigate the central nervous system changes induced by congenital Zika virus infection to better understand the spectrum of the changes they have seen.
"We are also interested in investigating how congenital Zika virus infection can interfere with not only prenatal, but also postnatal gray and white brain maturation," she added.
"Congenital Brain Abnormalities and Zika Virus: What the Radiologist Can Expect to See Prenatally and Postnatally." Collaborating with Drs. Tovar-Moll and Levine were Patricia Soares de Oliveira-Szejnfeld, M.D., Adriana Suely de Oliveira Melo, M.D., Ph.D., Melania Maria Ramos Amorim, M.D., Ph.D., Alba Gean M. Batista, M.D., Leila Chimelli, M.D., Ph.D., Amilcar Tanuri M.D., Ph.D., Renato Santana Aguiar, Ph.D., Gustavo Malinger, M.D., Renato Ximenes, M.D., M.Sc., Richard Robertson, M.D., and Jacob Szejnfeld, M.D., Ph.D.
The report provides an image-rich resource, including whole sequences of images of MRI and CT as movie files, for health care practitioners to allow them to become familiar with the spectrum of abnormalities seen with congenital Zika infection and can be found at http://radiology.rsna.org/.
Radiology is edited by Herbert Y. Kressel, M.D., Harvard Medical School, Boston, Mass., and owned and published by the Radiological Society of North America, Inc. (http://radiology.rsna.org/)
RSNA is an association of more than 54,000 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information CT and MRI of the brain and prenatal ultrasound, visit RadiologyInfo.org.
Images (.JPG and .TIF format) and Video clips (.mp4 format)
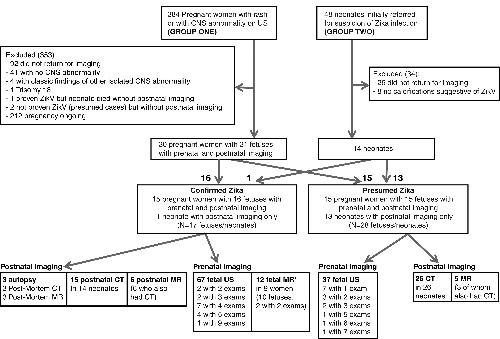
Figure 1: Flowchart for subject inclusion and exclusion in the confirmed and presumed Zika virus (ZikV) infection cohorts. ∗ = Gestational ages for fetal MR exam¬inations were 26 weeks (with a second MR examination at 30 weeks), 29 weeks, 29 weeks (with a second MR examination at 37 weeks), 32 weeks, 34 weeks, and four examinations at 36 weeks (one in a set of twins).
High-res (TIF) version
(Right-click and Save As)
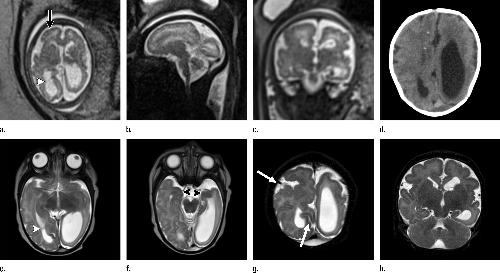
Figure 2. (a) Axial, (b) sagittal, and (c) coronal fetal T2-weighted MR images were obtained in a 29-year-old woman with confirmed Zika virus infection, initially seen for characteristic rash at 12 weeks of gestational age. (d) Axial postnatal CT image and (e–g) axial and (h) coronal T2-weighted MR images were obtained in her male neonate. The fetal MR images obtained at 34 weeks (a–c) show asymmetrical ventriculomegaly with a septation in the right occipital horn (arrowhead on a), small frontal lobes, thinning of the occipital parenchyma (left worse than right), underdeveloped sylvian fissures, and regions of thickened cortex, as in the right frontal lobe, which is suggestive of polymicrogyria (arrow on a). There is abnormal, increased signal intensity in the white matter. The postnatal CT image (d) obtained in the 22-day-old neonate shows punctate calcifications at the gray matter–white matter junction and asymmetrical ventriculomegaly. The T2-weighted MR images obtained at 26 days (e–h) show septation in the ventricle (arrowhead on e). Note how the right ventricle has relatively decreased in size compared with the prenatal image, whereas the left ventricle has increased in size. Under-rotation of the hippocampus (arrowheads on f) is demonstrated. There is clear asymmetry of the gyral pattern on g, which is relatively smooth in the left occipital region, with abnormal folds in the right occipital and frontoparietal regions (arrows on g). Subependymal cysts are visualized on h, which are not seen on fetal MR images.
High-res (TIF) version
(Right-click and Save As)
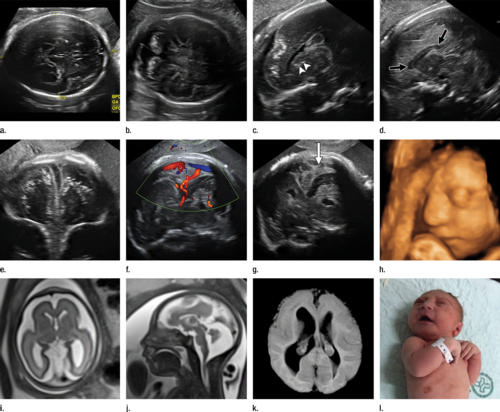
Figure 3. Images obtained in the case of a 34-year-old woman with confirmed Zika virus infection, initially seen for a rash at 8 weeks of gestation. Fetal head cir¬cumference was in the normal range at 12 and 16 weeks (5.8 cm and 11.9 cm, respectively) but then decreased to the 10th percentile at 22 weeks and was below the 3rd percentile in subsequent imaging examinations. (a–h) US images were obtained at 30 weeks. Head circumference on the axial image (a) measured 24 cm (˂2.3 percentile, corresponding to a gestational age of 26 weeks 3 days). Note the open sylvian fissures and relatively smooth cortex, which are abnormal findings at this gestational age. Oblique axial image (b) shows cerebellar calcifications (seen as the echogenic outer contour of the cerebellar hemispheres) and inferior vermian hypoplasia with associated enlarged cisterna magna. A sagittal transvaginal image (c) shows calcifications in the basal ganglia (arrowheads) and more bulky calcifi¬cation at the gray matter–white matter junction. Another sagittal transvaginal image (d) shows a relatively small corpus callosum (arrows). A coronal image (e) shows cortical and subcortical white matter calcifications in a linear pattern. The gyral pattern is abnormal, which is suggestive of polymicrogyria. A sagittal Color Doppler image (f) shows a stretched appearance of vessels coursing into the posterior fossa. An oblique axial grayscale transvaginal image in the posterior fossa (g) shows heterogeneous material in the confluence of sinuses due to blood clot (arrow). A three-dimensional US image of the face (h) shows a sloping forehead, compatible with frontal lobe hypoplasia. (i) Axial and (j) sagittal fetal MR images obtained at 29 weeks show atrophic frontal lobes, wide sylvian fissures, enlarged posterior fossa, abnormal gyral pattern, prominent cerebrospinal fluid spaces, and inferior vermian hypoplasia. On (i), note the diffuse hypointense and undersulcated cortex, which is suggestive of mineralization and polymicrogyria. The hypoplastic corpus callosum can be seen on the sagittal view (j), as well as the inferior vermian hypoplasia, en¬larged cisterna magna, and heterogeneous signal intensity in the confluence of sinuses. There is a subjectively thin spinal cord. (k) Postnatal axial MR image obtained at 81 days shows small frontal lobes and cortical thickening. The choroid plexi are enlarged. (l) Photograph of the neonate after birth.
High-res (TIF) version
(Right-click and Save As)

Figure 4. Images obtained in the case of an 18-year-old woman, first seen for rash at 10 weeks of pregnancy, with confirmed Zika virus infection. US findings obtained at 20 weeks of gestational age were reportedly normal, with normal head circumference of 17.5 cm. At 37 weeks of gestational age, (a) sagittal transvaginal and (b) coronal transabdominal US images obtained with the head upside down show a small head circumference (26.4 cm, corresponding to 28 weeks 5 days, below the 3rd percentile), moderate ventriculomegaly with dense intracranial calcifications (arrowheads on a), and abnormal head shape with flattened appearance and thickened skin (arrow on a). On the sonogram, it is difficult to precisely localize the calcifications, given the thin parenchyma. (c, d) Axial bone window CT images, (e) sagittal localizer CT image, and (f–h) axial CT images show microcephaly with cerebral atrophy, and, despite ventriculomegaly, the extra-axial cerebrospinal fluid spaces are still prominent. The hypoattenuating calcifications are predominantly located in the subcortical white matter at the gray matter–white matter interface. There is markedly abnormal skull shape with some eversion of the bones at the suture sites (particularly frontoparietal sites), with redundant skin folds (particularly in the parieto-occipital region). (i) Sagittal T1-weighted, (j, k) coronal T2-weighted, and (l) axial susceptibility-weighted MR images obtained at 1 month of age show an undersegmented midbrain, severe microcephaly, open sylvian fissures, and polymicrogyria. The dense calcifications are evident on the susceptibility-weighted image. On the sagittal images (a, e, i), note the small supratentorial compartment and associated skull deformity.
High-res (TIF) version
(Right-click and Save As)
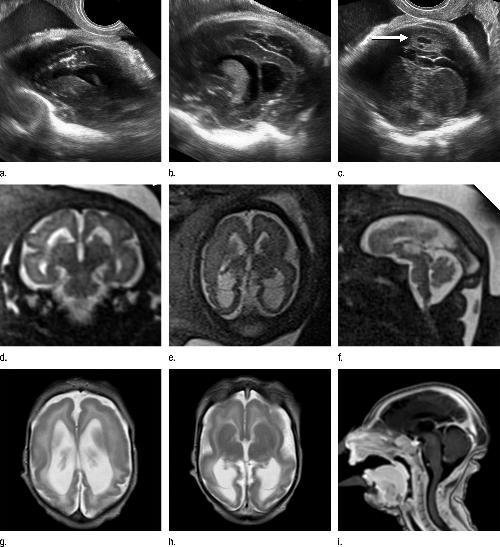
Figure 5. Images obtained in the case of a 33-year-old woman who had a rash at 10 weeks of pregnancy, with confirmed Zika virus infection. US performed at 19 weeks of gestational age showed a head circumference in the normal range (16.6 cm). (a, b) Sagittal and (c) coronal transvaginal US images obtained at the next US examination at 27 weeks 2 days of gestational age, however, showed the fetal head circumference to be 21.6 cm, which corresponded to 23 weeks 3 days (˂2.3 percentile, not shown). There was mild ven¬triculomegaly with septations in the occipital horns. Calcifications could be seen at the gray matter–white matter junction. The cerebrum was atrophic. There was blood clot in the region of the confluence of sinuses (arrow on c). (d) Coronal, (e) axial, and (f) sagittal T2- weighted fetal MR images obtained at 32 weeks show septations in the ventricles and an abnormal-appearing cortex, with a thickened and undersulcated cortex most marked on the left, compatible with polymicrogyria. The sagittal midline view shows microcephaly, blood clot in the region of the confluence of sinuses, and prominent skin folds. (g, h) Axial T2-weighted and (i) sagittal T1-weighted postnatal MR images obtained in the 4-week-old neonate show diffuse gyral abnormality and abnormal myelination. The septations in the ventri¬cles are again seen. The sagittal image shows thinning of the spinal cord at the craniocervical junction.
High-res (TIF) version
(Right-click and Save As)
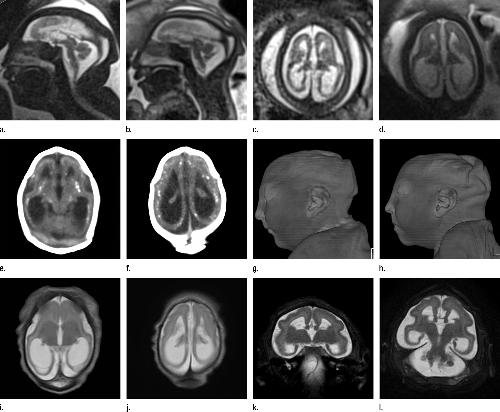
Figure 6. Images obtained in the case of a 24-year-old woman pregnant with twins, with characteristic rash at 9 weeks of pregnancy and confirmed Zika virus infection. (For each pair of images, the first image is of twin A, and the second image is of twin B.) At 14 weeks of gestational age, the fetal head size of both twins was normal. The head size never went below the 3rd percentile for either fetus in examinations at 19–28 weeks. (a, b) Sagittal and (c, d) axial fetal MR images were obtained at 36 weeks. (e, f) Axial and (g, h) surface reconstruction postnatal CT images and (i, j) axial T2-weighted and (k, l) coronal MR images were obtained 1 week after delivery at 38 weeks of gestational age. There is severe microcephaly with profound frontal lobe hypoplasia. Calcifications in the subcortical white matter at the gray matter–white matter junction are visualized. Both twins have a flattened appearance of the pons. The spinal cord is atrophic (best seen on a). Redundant skin is seen in the occipital region. There is polymicrogyria involving the frontal and parietal regions and atrophic cortex and white matter in the occipital regions. Each twin has hypoplasia of the corpus callosum, with prominent fornices. There is abnormal myelination in the occipital region that, in twin A (i), has the appearance of a cyst or septation within the ventricle. The cerebellum is somewhat small and nodular. There is lack of rotation of the hippocampi.
High-res (TIF) version
(Right-click and Save As)

Figure 7: Images obtained in the case of a pregnant 20-year-old woman, without history of rash, who was referred for fetal brain abnormality at US with confirmed Zika virus infection. (a) Graph of head circumference during pregnancy shows small head size in the second trimester, which increased in the third trimester. US (not shown) showed moderate ventriculomegaly starting at 23 weeks, which progressed to severe ventriculomegaly by the third trimester, associated with the increase in head circumference. (b) Axial, (c) sagittal, and (d) coronal fetal MR images obtained at 36 weeks show severe asymmetric ventriculomegaly, marked parenchymal thinning and/or atrophy, sloping forehead, and elevation of the hypoplastic cerebellar vermis with hypoplastic cerebellar hemispheres. The brainstem is thin, and the midbrain is foreshortened. The spinal cord is irregular, thin, and nonvisualized in parts, and then thicker and possibly mineralized. (e, f) Axial CT images obtained 1 day postnatally show severe asymmetrical ventriculomegaly with dense calcifications in the brainstem, cerebellum, and gray matter–white matter interface (temporal lobes on f) and marked parenchymal atrophy. (g) Axial CT image obtained in the 6-week-old infant, after shunting, showed persistent ventriculomegaly and periven¬tricular, midbrain, thalamic, and cerebellar calcifications. (h) Photograph of the neonatal face shows redundant skin folds and skull asymmetry.
High-res (TIF) version
(Right-click and Save As)

Figure 8: Fetal and postnatal images obtained in the case of an 18-year-old pregnant woman initially seen for a rash at 12 weeks of gestation, with confirmed Zika virus infection. Signs of joint contractures were identified at US at 17 weeks, but head circumference was in the normal range, then decreased to the 15th percentile at 21 weeks and was below the 3rd percentile at subsequent scans at 24 and 36 weeks (19.0 cm and 25.0 cm, respectively). (a) Axial transabdominal US performed at 36 weeks shows ventriculomegaly, calcifications in the thalamus and basal ganglia, and enlarged cisterna magna. (b) Soft-tissue, (c) body bone reconstruction, and (d, e) axial postmortem CT images show an abnormal profile, moderate ventriculomegaly, parenchymal atrophy, splaying of the cerebellar hemispheres, inferior vermian hypoplasia, and calcifications in the subcortical white matter, thalamus, and basal ganglia. The corpus callosum is not visualized. The gyral pattern is abnormally smooth for a term neonate. The postnatal bone reconstruction image showed the severe joint contractures, similar to those observed on (f) a photograph of the neonate.
High-res (TIF) version
(Right-click and Save As)

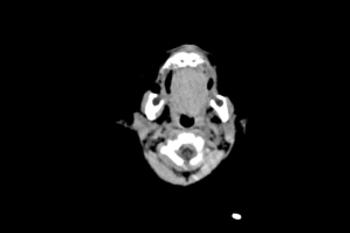
Figure 9: Axial CT image obtained in a 1-week-old female neonate with a head circumference of 31 cm at birth and presumed Zika virus infection. The frontal lobes are slightly hypoplastic, with mild underopercularization of the hypoplastic sylvian fis¬sures. There are scattered subcortical calcifications (arrowheads), and there is high-attenuating material (arrow) in the region of the confluence of sinuses, likely representing blood products.
High-res (TIF) version
(Right-click and Save As)
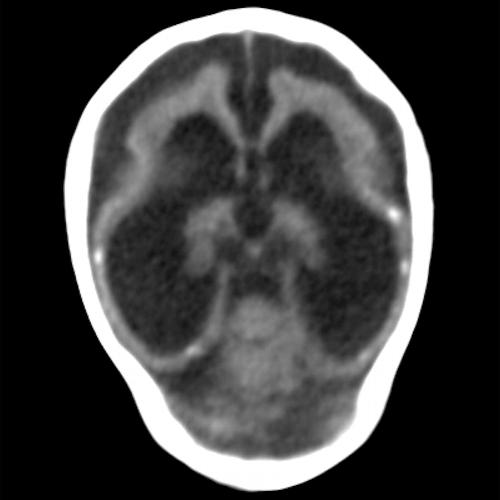
Figure 10: Oblique axial CT image obtained in a 3-month-old male infant with a head circumference of 27.5 cm at birth, with presumed Zika virus infection. Note the misshapen skull, ventriculomegaly, absent corpus callosum, diffuse parenchymal volume loss, diffuse cortical migrational abnormality, and calcifications, most likely subcortical but difficult to classify secondary to parenchymal thinning.
High-res (TIF) version
(Right-click and Save As)
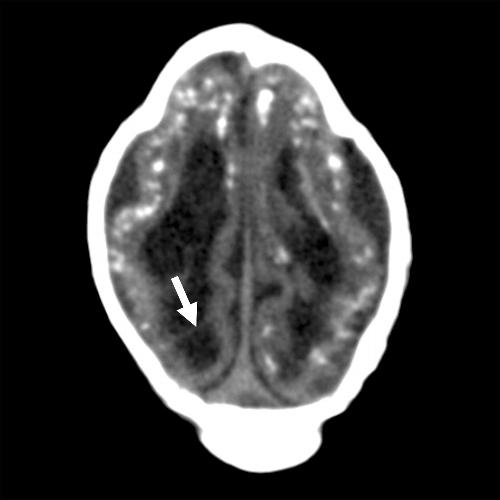
Figure 11: Axial CT image obtained in a 1-month-old male neonate with a head circumference of 27 cm at birth, with presumed Zika virus infection. Note ventriculomegaly with septation (arrow) in the right occipital horn and striking subcortical calcifications. There are also cortical and periventricular calcifica-tions. The gyral pattern is diffusely abnormal, and the skull is deformed.
High-res (TIF) version
(Right-click and Save As)

Figure 12: Oblique coronal CT image obtained in a 1-month-old male neonate with a head circumfer¬ence of 29.5 cm at birth, with presumed Zika virus infection. Note the misshapen skull; ventriculomeg¬aly; absent corpus callosum; cerebellar hypoplasia (arrows); thin parenchyma with diffuse gyral abnormality; calcifications in the thalamus, basal ganglia, and subcortical white matter; and cerebellar hemispheres.
High-res (TIF) version
(Right-click and Save As)
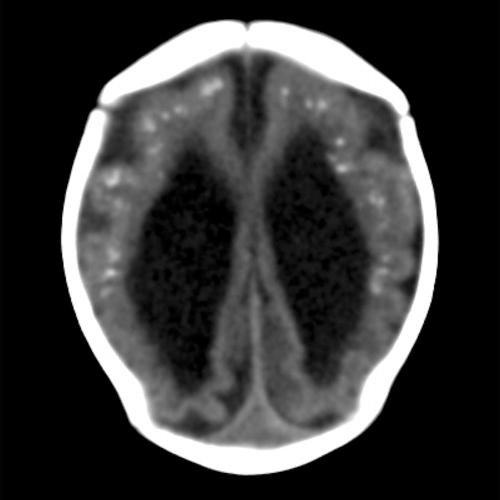
Figure 13: Axial CT image obtained in a 1-month-old female neonate with a head circumference of 31 cm at birth, with presumed Zika virus infection. Note severe ventriculomegaly, subcortical calcifications, and diffuse gyral abnormality.
High-res (TIF) version
(Right-click and Save As)
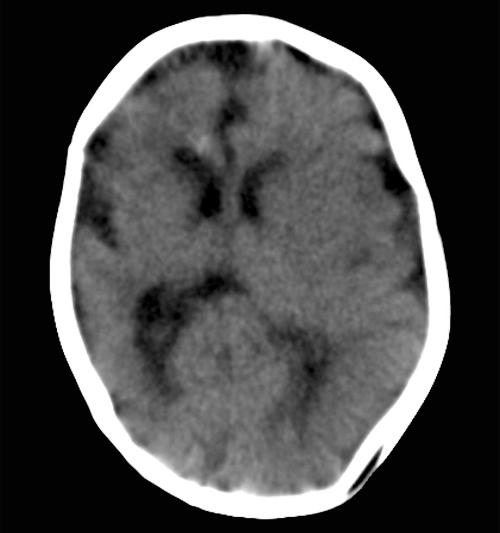
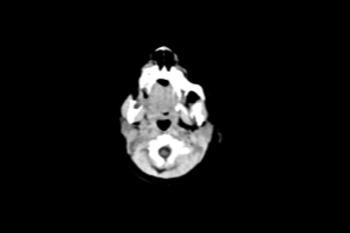
Figure 14: Axial CT image obtained in a 2-month-old female infant with a head circumference of 32.5 cm at birth, with presumed Zika virus infection. Note the asymmetrical volume loss, more marked on the right than the left. Also note the diffusely irregular sulci and gyri bilaterally.
High-res (TIF) version
(Right-click and Save As)

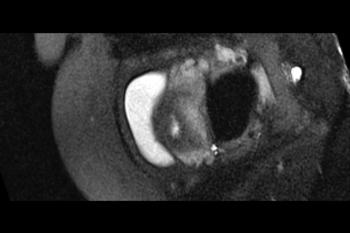
Figure 15: Axial CT image obtained in a 3-month-old female infant with cord blood positive for Zika virus (confirmed Zika virus infection) and a head circum¬ference of 28.5 cm at birth. The mother had a rash at 12 weeks. Bilateral cataracts are seen, as well as abnormal cerebellar vermis and fat herniating posteriorly from the orbits through the superior orbital fissure into the cranial vault.
High-res (TIF) version
(Right-click and Save As)
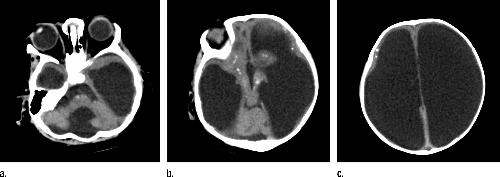
Figure 16: (a–c) Axial CT images obtained in a 5-month-old male infant with a head circumference of 38 cm at birth. The mother had a rash at 11 weeks. The size of the head is likely secondary to hydrocephalus. Unlike most of our cohort, the head was still round in shape. However, calcifications are present in the subcortical region, thalamus, basal ganglia, and brainstem. No sulci were seen; how-ever, the parenchyma is extremely thin. There is pontocerebellar hypoplasia, nonvisualization of the corpus callosum, and Dandy-Walker spectrum anomaly. This is an example of how Zika virus infection can be missed if only newborns with microcephaly are assessed.
High-res (TIF) version
(Right-click and Save As)
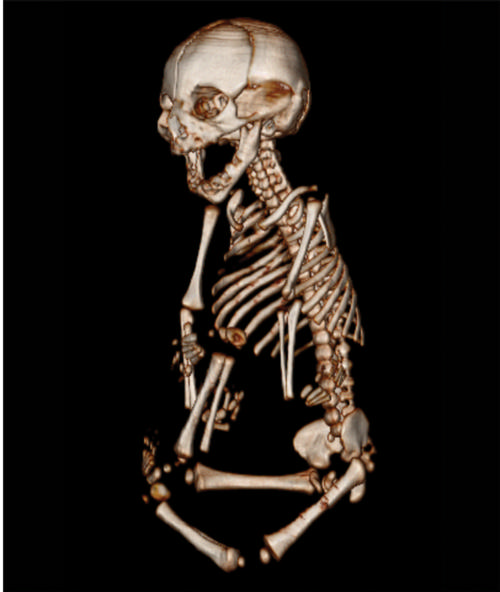
Figure 17: Fetal image showing body bone reconstruction obtained in the case of an 18-year-old pregnant woman initially seen for a rash at 12 weeks of gestation, with confirmed Zika virus infection.
High-res (TIF) version
(Right-click and Save As)

Figure 18: A three-dimensional US image obtained at 30 weeks in the case of a 34-year-old woman with confirmed Zika virus infection, initially seen for a rash at 8 weeks of gestation. Image of the face shows a sloping forehead, compatible with frontal lobe hypoplasia.
High-res (TIF) version
(Right-click and Save As)

Figure 19: Image obtained at 29 weeks in the case of a 34-year-old woman with confirmed Zika virus infection, initially seen for a rash at 8 weeks of gestation. Sagittal fetal MR images show atrophic frontal lobes, wide sylvian fissures, enlarged posterior fossa, abnormal gyral pattern, prominent cerebrospinal fluid spaces, and inferior vermian hypoplasia. The hypoplastic corpus callosum can be seen, as well as the inferior vermian hypoplasia, enlarged cisterna magna, and heterogeneous signal intensity in the confluence of sinuses. There is a subjectively thin spinal cord.
High-res (TIF) version
(Right-click and Save As)

Figure 20: Case of a 34-year-old woman with confirmed Zika virus infection, initially seen for a rash at 8 weeks of gestation. Photograph of the neonate after birth.
High-res (TIF) version
(Right-click and Save As)
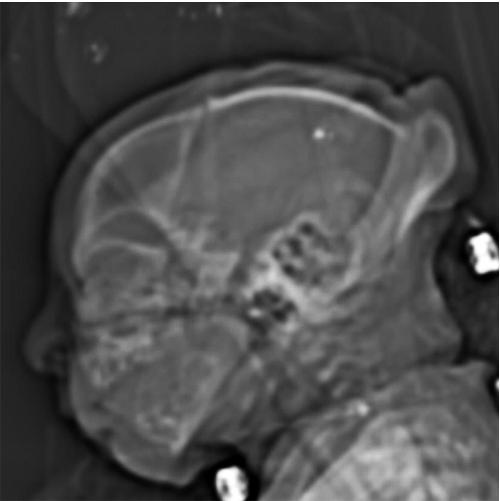
Figure 21: Image obtained at 37 weeks in the case of an 18-year-old woman, first seen for rash at 10 weeks of pregnancy, with confirmed Zika virus infection. US findings obtained at 20 weeks of gestational age were reportedly normal, with normal head circumference of 17.5 cm. Sagittal localizer CT image shows microcephaly with cerebral atrophy, and, despite ventriculomegaly, the extra-axial cerebrospinal fluid spaces are still prominent. Note the small supratentorial compartment and associated skull deformity.
High-res (TIF) version
(Right-click and Save As)
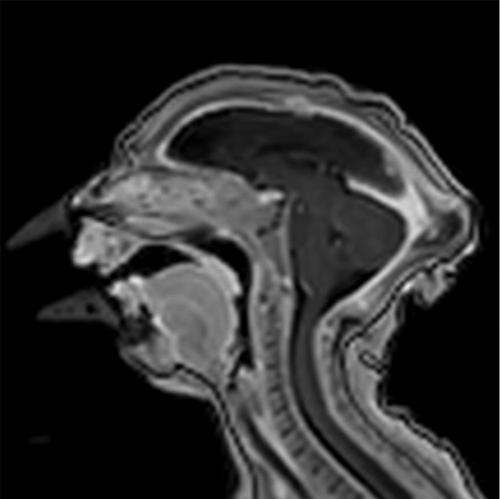
Figure 22: Image obtained at 1 month of age in the case of an 18-year-old woman, first seen for rash at 10 weeks of pregnancy, with confirmed Zika virus infection. US findings obtained at 20 weeks of gestational age were reportedly normal, with normal head circumference of 17.5 cm. Sagittal T1-weighted image shows an undersegmented midbrain, severe microcephaly, open sylvian fissures, and polymicrogyria. Note the small supratentorial compartment and associated skull deformity.
High-res (TIF) version
(Right-click and Save As)
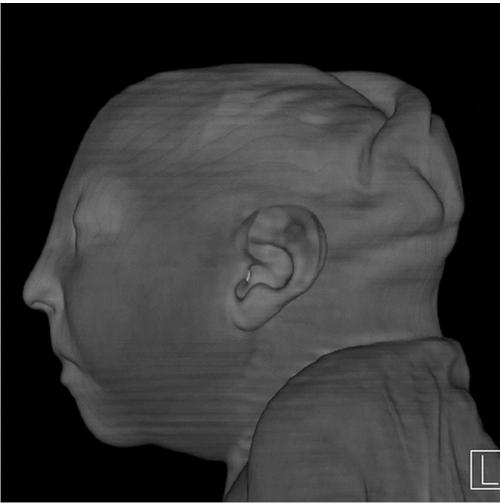
Figure 23: Surface reconstruction postnatal CT image obtained 1 week after delivery at 38 weeks of gestational age in the case of a 24-year-old woman pregnant with twins, with characteristic rash at 9 weeks of pregnancy and confirmed Zika virus infection.
High-res (TIF) version
(Right-click and Save As)
Video (.mp4 format)
Video (.mp4 format)
Video (.mp4 format)
Video (.mp4 format)
Video (.mp4 format)