RSNA Press Release
- Results from a multicenter trial show that BI-RADS 3 breast lesions have a low malignancy rate and could be re-evaluated with follow-up imaging in 12 months.
- BI-RADS 3 lesions are common on screening ultrasound and often lead to unnecessary biopsies and additional testing.
- The malignancy rate of BI-RADS 3 lesions in the study was 0.8%.
Multicenter Trial Finds Screening Ultrasound-Detected BI-RADS 3 Breast Lesions Have Low Cancer Rate
Released: August 20, 2013
| Media Contacts: | |
| RSNA Media Relations: | 1-630-590-7762 |
| Linda Brooks 1-630-590-7738 lbrooks@rsna.org |
Maureen Morley 1-630-590-7754 mmorley@rsna.org |
OAK BROOK, Ill. — Based on data from a multi-site imaging trial involving more than 2,600 women, researchers say breast lesions categorized as 'probably benign' on supplemental screening ultrasound could be re-evaluated with imaging in 12 months, reducing patient anxiety, follow-up exams and unnecessary biopsies. Results of the study are published online in the journal Radiology.
In the study, a team of researchers analyzed data from the American College of Radiology Imaging Network (ACRIN) trial 6666, in which both annual mammography and ultrasound screenings were performed on women with dense breasts at 21 sites around the country. Ultrasound is increasingly being used as a supplement to screening mammography because it is able to detect breast cancers that may not be visible with mammography, especially in dense breasts.
"Supplemental ultrasound screening increases cancer detection beyond mammography alone, but may also result in an increased number of additional tests," said lead researcher Richard G. Barr, M.D., Ph.D., professor of radiology at the Northeast Ohio Medical University in Youngstown, Ohio. "Both screening ultrasound and screening mammography have similar issues: to find breast cancers, a large number of biopsies must be performed, most of which turn out to be negative."

Dr. Barr and colleagues analyzed the trial's ultrasound-detected lesions assessed as probably benign or category 3 of the Breast Imaging-Reporting and Data System (BI-RADS), a standardized system of assessing breast lesions and their probability of malignancy based on appearance, to determine the prevalence and malignancy rate of these lesions.
Guidelines suggest that BI-RADS 3 lesions should be monitored for suspicious changes with additional imaging at intervals of six, 12 and 24 months.
"BI-RADS 3 lesions are common on screening ultrasound and often lead to unnecessary biopsies and additional imaging, causing substantial cost and anxiety for patients," Dr. Barr said. "We wanted to study these BI-RADS 3 lesions to look for ways to perform fewer biopsies without missing breast cancers."
The researchers analyzed the screening ultrasound exams and follow-up data of 2,662 trial participants recruited between 2004 and 2006. Of the 2,662 women, 519 had a total of 745 BI-RADS 3 lesions, representing 25 percent of all ultrasound-detected lesions in the study.
Of the 745 BI-RADS 3 lesions, six were malignant for a total malignancy rate of 0.8 percent. The average size of the detected cancers among the BI-RADS 3 lesions was 10 millimeters.
During six-month follow-up imaging, suspicious changes were observed in only one of the 745 BI-RADS 3 lesions. At 12-month follow-up imaging, suspicious changes were observed in a second BI-RADS 3 lesion, revealing an invasive breast cancer that had not yet spread beyond the breast.
"As a result of the low malignancy rate of BI-RADS 3 lesions and the low rate of suspicious changes at six-month follow-up imaging, yearly follow-up for these lesions may be appropriate," Dr. Barr said. "The cancers detected due to changes at one year had not spread beyond the breast, with similar prognosis if the lesion was biopsied on initial detection."
Dr. Barr said extending the follow-up imaging interval from six to 12 months for BI-RADS 3 lesions detected by screening ultrasound would substantially decrease the number of follow-up examinations and biopsies performed.
The researchers also found that women in the study with BI-RADS 3 lesions were more likely to be younger than 50 years of age, of Hispanic or Latino ethnicity and pre-menopausal.
Dr. Barr is currently conducting additional studies on ultrasound screening and research on the use of elastography, an advanced technique that helps distinguish benign from cancerous lesions.
# # #
"Probably Benign Lesions at Screening Breast US in a Population with Elevated Risk: Prevalence and Rate of Malignancy in the ACRIN 6666 Trial." Collaborating with Dr. Barr were Zheng Zhang, Ph.D., Jean B. Cormack, Ph.D., Ellen B. Mendelson, M.D., and Wendie A. Berg, M.D., Ph.D. The Avon Foundation and grants from the National Cancer Institute funded the study.
Radiology is edited by Herbert Y. Kressel, M.D., Harvard Medical School, Boston, Mass., and owned and published by the Radiological Society of North America, Inc. (http://radiology.rsna.org/)
RSNA is an association of more than 51,000 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on breast ultrasound, visit RadiologyInfo.org.
Images
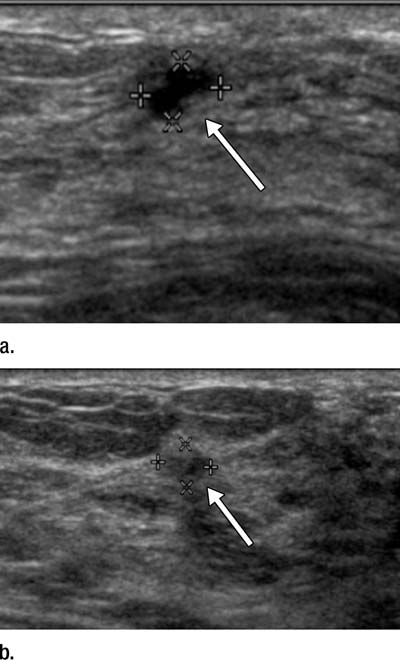 Figure 1: (a, b) Sonograms show a BI-RADS category 3 lesion (arrow) in a woman aged 43 years at 1-year follow-up. (a) This lesion was described as 5-mm clustered microcysts at 1-year follow-up. (b) At 2-year follow-up, the lesion had suspicious changes and was reclassified as a BI-RADS cate¬gory 4a solid lesion. The lesion was not detected with mammography in either year. At biopsy, the lesion was determined to be an 18-mm invasive lobular cancer (N0). High-res (TIF) version (Right-click and Save As) |
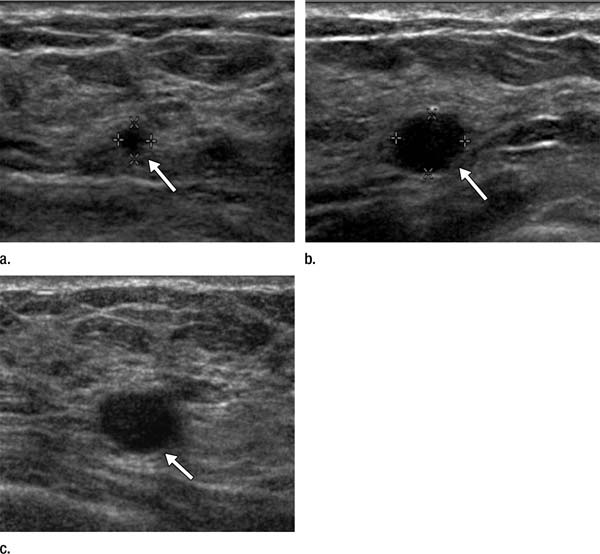 Figure 2: (a) At year 1 screening US, a 4-mm circumscribed oval mass (arrow) was described in a 59-year-old woman and assessed as a BI-RADS category 3 lesion. (b, c) The lesion (arrow) increased in size to (b) 8 mm in year 2 and (c) 12 mm in year 3. It was classified as a BI-RADS category 4a lesion in year 3. This lesion was not detected at mammography until year 3. At patho¬logic analysis, the lesion was determined to be a 12-mm grade 2 IDC with associated DCIS with a metastatic axillary node (N1). High-res (TIF) version (Right-click and Save As) |
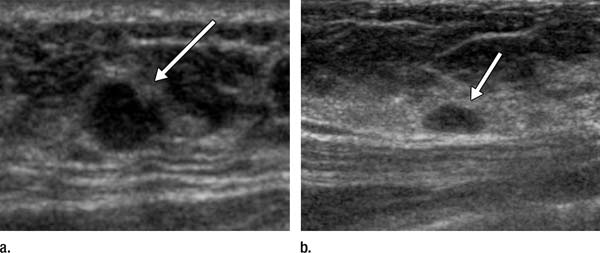 Figure 3: (a, b) US images in a 46-year-old woman with a BI-RADS category 4C lesion in her right breast that was classified as grade 3 invasive ductal cancer at pathologic analysis. At screening US, she also had a 7-mm right breast lesion (arrow in b) and a 7-mm left breast lesion (arrow in a), both of which were classified as BI-RADS category 3; these lesions were not detected at mammography. She elected to undergo bilateral mastectomy (prophylactic on the left side). On the basis of lesion locations, the lesion in the left breast (a) was thought to correlate with DCIS (NX), whereas the lesion in the right breast (b) was thought to correlate with a 10-mm IDC with associated DCIS (N0). High-res (TIF) version (Right-click and Save As) |
 PDF
PDF{kind=link}