RSNA Press Release
- Screening with MRI is highly accurate in women with a personal history of treated breast cancer.
- Breast MRI identified more cancers with fewer false positives in women with a personal history of breast cancer than in women with a genetic or family history of breast cancer.
- The American Cancer Society currently recommends annual screening with breast MRI for women with a genetic or family history of breast cancer but does not recommend for or against MRI screening for women with a personal history of breast cancer.
Women With Personal History of Breast Cancer Should be Screened With MRI
Released: November 29, 2010
| Media Contacts: | RSNA Newsroom | 1-312-949-3233 |
| Before 11/27/2010 or after 12/02/2010: | RSNA Media Relations: | 1-630- 590-7762 |
| |
Linda Brooks 1-630-590-7738 lbrooks@rsna.org |
Maureen Morley 1-630-590-7754 mmorley@rsna.org |
CHICAGO — Women with a personal history of breast cancer should consider annual screening with MRI in addition to mammography, according to a study presented today at the annual meeting of the Radiological Society of North America (RSNA).
The American Cancer Society (ACS) guidelines currently recommend annual screening with breast MRI in women with a known gene mutation or with a strong family history indicating a lifetime risk of breast cancer greater than 20 percent. However, the guidelines say there is insufficient evidence to recommend for or against MRI screening in women who have already had breast cancer themselves.
"In our study using breast MRI screening, we actually detected proportionally more cancers in women with a personal history of breast cancer, compared with those women with a genetic mutation or strong family history who are currently recommended to have breast MRI," said Wendy B. DeMartini, M.D., assistant professor in the Department of Radiology at the University of Washington Medical Center and Seattle Cancer Care Alliance in Seattle. "Further, women with a personal history were less likely to be recalled for additional testing and less likely to have a biopsy for a false positive MRI finding."
Dr. DeMartini and colleagues performed a retrospective review of initial screening breast MRI examinations of 1,026 women from January 2004 to June 2009. Of the 1,026 women, 327 had a genetic or family history of breast cancer and 646 had a personal history of treated breast cancer.
Overall, MRI testing identified 25 of 27 cancers in the group for a sensitivity rate of 92.6 percent.
The cancer yield in the women with a personal history of breast cancer (3.1 percent) was double that of the women with a genetic or family history (1.5 percent). Specificity in women with a personal history was 93.6 percent, compared with 86.3 percent for the other group. Specificity refers to the accuracy of the exam in correctly ruling out cancer where it is not present, resulting in lower recall and biopsy rates due to false-positive findings.
Biopsy was recommended in 9.3 percent of the women with a personal history of breast cancer, compared with 15 percent of the genetic and family history group. The positive predictive value of biopsy was also higher in the personal history group, with 35.7 percent of biopsies yielding cancer, compared with only 12.2 percent in the other group.
"Our findings show that the diagnostic performance of MRI in patients with a personal history of treated breast cancer supports consideration of screening MRI as an adjunct to mammography," Dr. DeMartini said. "Additional studies such as ours are necessary to establish guidelines for screening this important group of women."
Coauthors are Grace Kalish, M.D., Sue Peacock, M.Sc., Peter Eby, M.D., Robert Gutierrez, M.D., and Constance Lehman, M.D., Ph.D.
# # #
Note: Copies of RSNA 2010 news releases and electronic images will be available online at RSNA.org/press10 beginning Monday, Nov. 29.
RSNA is an association of more than 44,000 radiologists, radiation oncologists, medical physicists and related scientists committed to excellence in patient care through education and research. The Society is based in Oak Brook, Ill. (RSNA.org)
Editor's note: The data in these releases may differ from those in the printed abstract and those actually presented at the meeting, as researchers continue to update their data right up until the meeting. To ensure you are using the most up-to-date information, please call the RSNA Newsroom at 1-312-949-3233.
For patient-friendly information on breast MRI, visit RadiologyInfo.org.
| Abstract: |
Images (.JPG format)
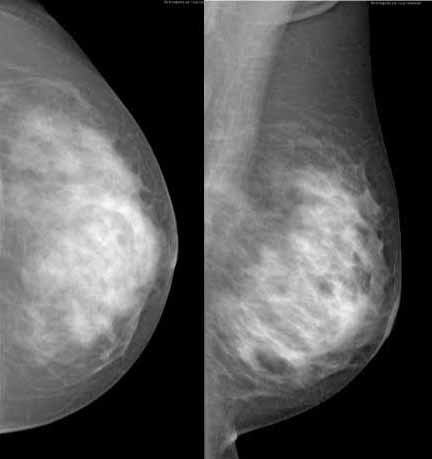
Figure 1a: Mammography images from an asymptomatic 38-year-old woman with a history of prior right breast invasive cancer, treated with mastectomy and chemotherapy six years ago. These images of the left breast demonstrate dense breast tissue and no abnormality. High-res (TIF) version (Right-click and Save As) |

Figure 1b: Breast MR image from an asymptomatic 38-year-old woman with a history of prior right breast invasive cancer, treated with mastectomy and chemotherapy six years ago. This image (following contrast) demonstrates an enhancing 15 mm irregular mass (arrow) in the left breast, not noticeable on the mammogram. Subsequent biopsy of the mass was performed under MR guidance and yielded invasive breast cancer. The right breast demonstrates normal findings of mastectomy with implant reconstruction. High-res (TIF) version (Right-click and Save As) |
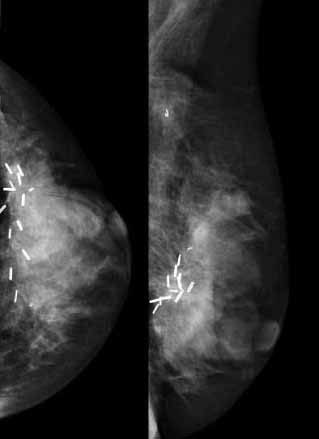
Figure 2a: Mammography images from an asymptomatic 50-year-old woman with a history of prior left breast invasive cancer, treated with lumpectomy, radiation therapy and chemotherapy approximately one year ago. Screening mammogram images of the left breast demonstrate dense breast tissue, multiple surgical clips at the lumpectomy site, and no abnormality. High-res (TIF) version (Right-click and Save As) |
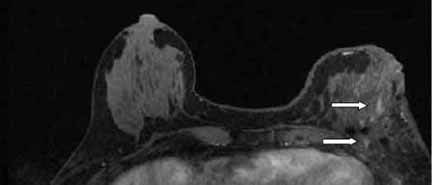
Figure 2b: Breast MR image from an asymptomatic 50-year-old woman with a history of prior left breast invasive cancer, treated with lumpectomy, radiation therapy and chemotherapy approximately one year ago. This image (following contrast) demonstrates a 40 mm enhancing area (arrows) in the left breast, not noticeable on the mammogram. The abnormality surrounds the lumpectomy site surgical clips. Subsequent biopsy of the area was performed under MR guidance and yielded invasive breast cancer. The right breast demonstrates no abnormality. High-res (TIF) version (Right-click and Save As) |
 PDF
PDF