Radiologist Recommendations for Chest CT Have High Clinical Yield
Released: December 22, 2014
At A Glance
- Radiologist-recommended chest CTs to evaluate abnormal findings on outpatient chest X-rays result in a high yield of clinically relevant findings.
- Of the outpatient chest X-ray reports studied, 4.5% contained a recommendation for chest CT.
- Of chest CTs performed within one year of the recommendation, 41.4% showed a corresponding abnormality that required treatment or further diagnostic work-up and 8.1% revealed a newly-diagnosed, biopsy-proven malignancy.
- RSNA Media Relations
1-630-590-7762
media@rsna.org
OAK BROOK, Ill.—A substantial percentage of patients who receive radiologist recommendations for chest computed tomography (CT) to evaluate abnormal findings on outpatient chest X-rays have clinically relevant findings, including cancer, according to a new study published online in the journal Radiology.
Researchers said the findings show that radiologist recommendations for additional imaging (RAIs) after chest X-rays represent valuable contributions to patient care.
RAIs, which have grown 200 percent since 1995, have attracted scrutiny in recent years as healthcare moves from volume-driven to value-based payment models. The scrutiny makes it increasingly important for the radiology community to validate the clinical impact of its work, said study author Tarik K. Alkasab, M.D., Ph.D., from Massachusetts General Hospital and Harvard Medical School in Boston.
"There has been a great deal of research on how radiologists recommend an imaging exam, but little on what comes out of the exams that they recommend," Dr. Alkasab said. "Prior studies were very broad, so in our study we tried to focus on a specific clinical scenario."
Dr. Alkasab and colleagues looked at chest X-rays, one of the most common outpatient diagnostic imaging studies performed in the United States. As many as half of all RAIs arising from thoracic diagnostic exams are prompted by chest X-rays.
The researchers combed through more than 29,000 reports of outpatient chest X-rays performed at a large academic center over one year to identify studies that included a recommendation for a chest CT. They found that radiologists interpreting outpatient chest X-rays made recommendations for CT in 4.5 percent of cases—a result in line with existing research. Increasing patient age and positive smoking history were associated with an increased likelihood of a chest CT recommendation.
When the researchers looked at the chest CTs obtained within one year of the index chest X-ray, they found that 41.4 percent detected a corresponding abnormality requiring treatment or further diagnostic workup. One in every 13 yielded a corresponding abnormality representing a newly-diagnosed, biopsy-proven malignancy.
"In this era of concern about radiation dose risk, these findings suggest that the extremely low predicted risk of radiation-induced cancer associated with a chest CT is orders of magnitude less than the potential clinical benefits," said study co-author H. Benjamin Harvey, M.D., J.D., from Massachusetts General Hospital and Harvard Medical School. "If ordering physicians see a recommendation for chest CT, they need to ensure that the patient gets the recommended imaging."
More than one-third of patients in the study group who were recommended for follow-up chest CT did not receive the exam within one year—an oversight that could result in missed or delayed diagnoses, the researchers said.
"More research is needed to understand the possible reasons for the less-than-optimal adherence to RAIs after chest X-ray," Dr. Harvey said. "One thing we're looking at is how the recommendation language affects recommendation adherence."
The researchers hope that their study helps improve awareness of the importance of follow-up CT.
"These results show that radiologists should be confident their recommendations are adding value and protecting patients," Dr. Alkasab said.
"Diagnostic Yield of Recommendations for Chest CT Examination Prompted by Outpatient Chest Radiographic Findings." Collaborating with Drs. Alkasab and Harvey were Matthew D. Gilman, M.D., Carol C. Wu, M.D., Matthew S. Cushing, M.D., Elkan F. Halpern, Ph.D., Jing Zhao, Ph.D., Pari V. Pandharipande, M.D., MPH, and Jo-Anne O. Shepard, M.D.
Radiology is edited by Herbert Y. Kressel, M.D., Harvard Medical School, Boston, Mass., and owned and published by the Radiological Society of North America, Inc. (Radiology.RSNA.org)
The Radiological Society of North America (RSNA) is an association of more than 54,000 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on chest X-ray and chest CT, visit RadiologyInfo.org.
Images (.JPG and .TIF format)
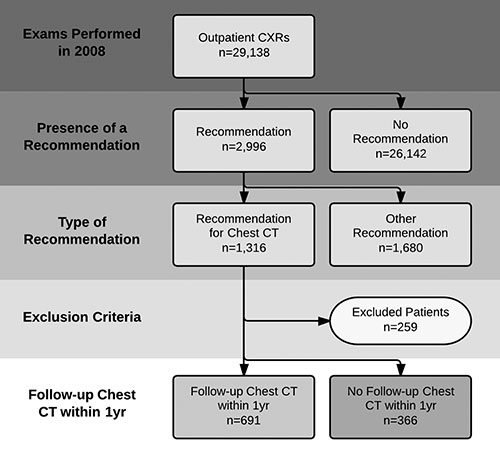
Figure 1. Schematic representation of the patient selection process. CXR = chest radiographic examination.
High-res (TIF) version
(Right-click and Save As)
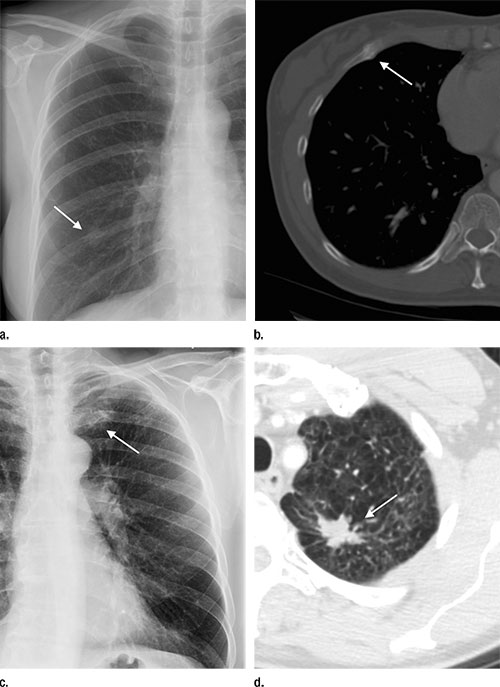
Figure 2. Examples of lesions seen on chest radiographic images that prompted a recommendation for chest CT examination and the corresponding abnormality on chest CT. (a, b) In the first example, a nodular opacity (arrow on a) is seen projecting over the right posterior ninth rib in the chest radiographic image of a 50-year-old woman who presented with cough; the recommended chest CT examination demonstrated this to be callus from a remote rib fracture (arrow on b). (c, d) In the second example, a nodular opacity (arrow in c) is seen projecting over the left anterior first rib on the chest radiographic image of a 53-year-old man who is a former smoker and presented with cough; the recommended chest CT examination demonstrated this to be a suspicious nodule in the apicoposterior segment of the left upper lobe (arrow in d). On resection, this was found to be well-differentiated adenocarcinoma of the lung.
High-res (TIF) version
(Right-click and Save As)
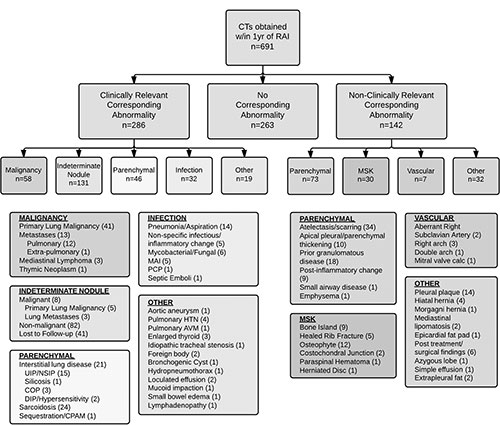
Figure 3. Schematic representation of the results of follow-up chest CT examinations performed within 1 year of the index outpatient chest radiographic examinations that contained the RAI. AVM = arteriovenous malformation, calc = calcification, COP = cryptogenic organizing pneumonia, CPAM = congenital pulmonary airways malformation, DIP = desquamative interstitial pneumonia, HTN = hypertension, MAI = Mycobacterium avium intracellulare, MSK = musculoskeletal, NSIP = nonspecific interstitial pneumonia, PCP = Pneumocystis pneumonia, UIP = usual interstitial pneumonia.
High-res (TIF) version
(Right-click and Save As)