Groups Publish Statements on CT Contrast Use in Patients with Kidney Disease
Released: January 21, 2020
At A Glance
- New consensus statements address the risk of intravenous iodinated contrast media in patients with impaired kidney function.
- The ACR-NKF statements say risk has been overstated due to the conflation of contrast-induced injury and contrast-associated injury.
- The statements answer key questions and provide recommendations for contrast use in patients impaired kidney function.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Dionna Arnold
1-630-590-7791
darnold@rsna.org
OAK BROOK, Ill. — The risk of administering modern intravenous iodinated contrast media in patients with reduced kidney function has been overstated, according to new consensus statements from the American College of Radiology (ACR) and the National Kidney Foundation (NKF), jointly published in the journals Radiology and Kidney Medicine.

{kind=link}
Intravenous iodinated contrast media are commonly used with computed tomography (CT) to evaluate disease and to determine treatment response. Although patients have benefited from their use, iodinated contrast media have been denied or delayed in patients with reduced kidney function due to the perceived risks of contrast-induced acute kidney injury. This practice can hinder a timely and accurate diagnosis in these patients.
"The historical fears of kidney injury from contrast-enhanced CT have led to unmeasured harms related to diagnostic error and diagnostic delay," said lead author Matthew S. Davenport, M.D., associate professor of radiology and urology at the University of Michigan in Ann Arbor, Michigan. "Modern data clarify that this perceived risk has been overstated. Our intent is to provide multi-disciplinary guidance regarding the true risk to patients and how to apply a consideration of that risk to modern clinical practice."
These consensus statements were developed to improve and standardize the care of patients with
impaired kidney function who may need to undergo exams that require intravenous iodinated contrast media to provide the clearest images and allow for the most informed diagnosis.
In clinical practice, many factors are used to determine whether intravenous contrast media should be administered. These include probability of an accurate diagnosis, alternative methods of diagnosis, risks of misdiagnosis, expectations about kidney function recovery, and risk of allergic reaction. Decisions are rarely based on a single consideration, such as risk of an adverse event specifically related to kidney impairment. Consequently, the authors advise that these statements be considered in the context of the entire clinical scenario.
Importantly, the report outlines the key differences between contrast-induced acute kidney injury (CI-AKI) and contrast-associated acute kidney injury (CA-AKI). In CI-AKI, a causal relationship exists between contrast media and kidney injury, whereas in CA-AKI, a direct causal relationship has not been demonstrated. The authors suggest that studies that have not properly distinguished the two have contributed to the overstatement of risk.
"A primary explanation for the exaggerated perceived nephrotoxic risk of contrast-enhanced CT is nomenclature," Dr. Davenport said. "'Contrast-induced' acute kidney injury implies a causal relationship. However, in many circumstances, the diagnosis of CI-AKI in clinical care and in research is made in a way that prevents causal attribution. Disentangling contrast-induced AKI (causal AKI) from contrast-associated AKI (correlated AKI) is a critical step forward in improving understanding of the true risk to patients."
The statements answer key questions and provide recommendations for use of intravenous contrast media in treating patients with varying degrees of impaired kidney function.
Although the true risk of CI-AKI remains unknown, the authors recommend intravenous normal saline for patients without contraindication, such as heart failure, who have acute kidney injury or an estimated glomerular filtration rate (eGFR) less than 30 mL/min per 1.73 m2 who are not undergoing maintenance dialysis. In individual and unusual high-risk circumstances (patients with multiple comorbid risk factors), prophylaxis may be considered in patients with an eGFR of 30–44 mL/min per 1.73 m2 at the discretion of the ordering clinician.
The presence of a solitary kidney should not independently influence decision making regarding the risk of CI-AKI. Lowering of contrast media dose below a known diagnostic threshold should be avoided due to the risk of lowering diagnostic accuracy. Also, when feasible, medications that are toxic to the kidneys should be withheld by the referring clinician in patients at high risk. However, renal replacement therapy should not be initiated or altered solely based on contrast media administration.
The authors emphasize that prospective controlled data are needed in adult and pediatric populations to clarify the risk of CI-AKI.
"Use of Intravenous Iodinated Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation." Collaborating with Dr. Davenport were Mark A. Perazella, M.D., Jerry Yee, M.D., Jonathan R. Dillman, M.D., M.S., Derek Fine, M.D., Robert J. McDonald, M.D., Ph.D., Roger A. Rodby, M.D., Carolyn L. Wang, M.D., and Jeffrey C. Weinreb, M.D.
Radiology is edited by David A. Bluemke, M.D., Ph.D., University of Wisconsin School of Medicine and Public Health, Madison, Wis., and owned and published by the Radiological Society of North America, Inc. (https://pubs.rsna.org/journal/radiology)
RSNA is an association of over 53,400 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on contrast materials, visit RadiologyInfo.org.
Images (.JPG and .TIF format)
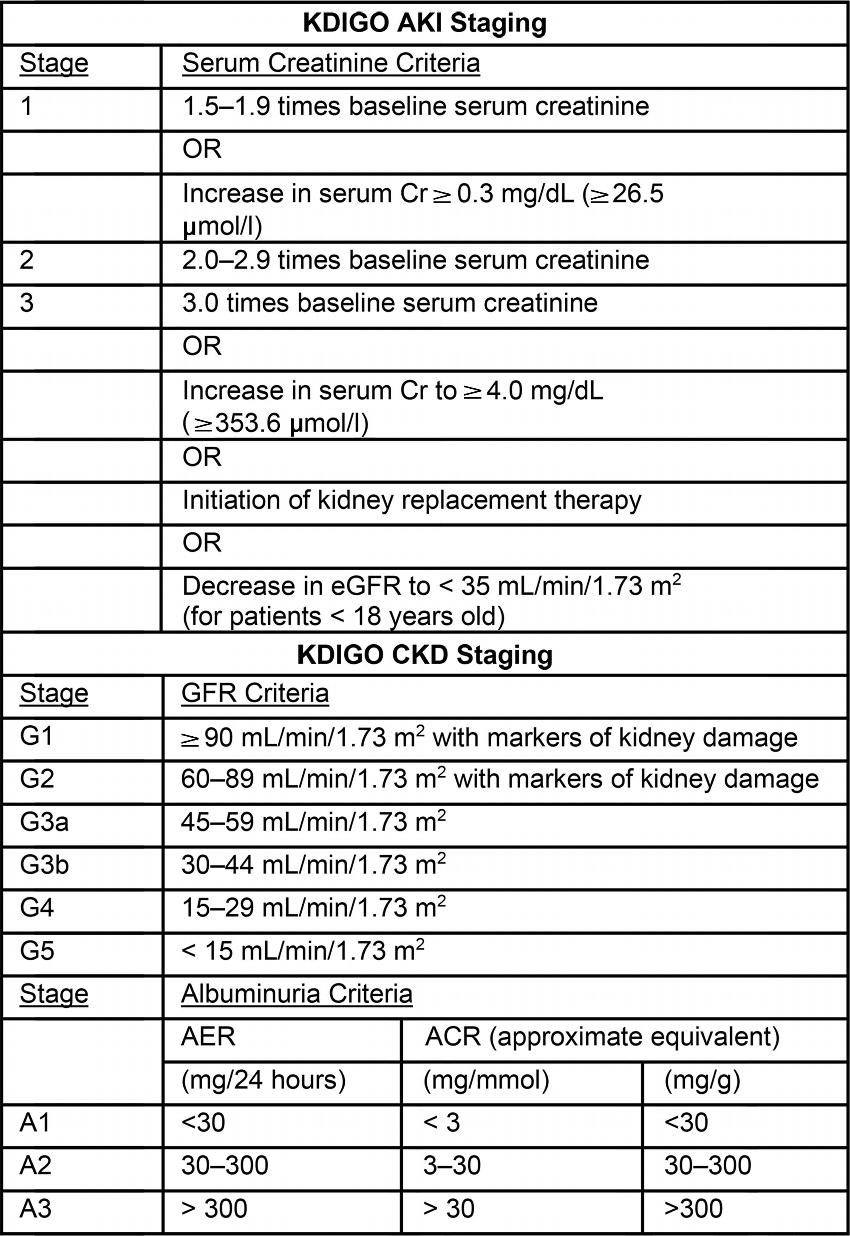
Figure 1. Image shows Kidney Disease Improving Global Outcomes (KDIGO) staging criteria for acute kidney injury (AKI) and chronic kidney disease (CKD). Urine output criteria for AKI staging were not included. ACR = albumin creatinine ratio, AER = albumin excretion rate, Cr = creatinine, GFR = glomerular filtration rate.
High-res (TIF) version
(Right-click and Save As)