Deep Learning Assists in Detecting Malignant Lung Cancers
Released: November 12, 2019
At A Glance
- Assisted by deep-learning based software, radiologists were better able to detect malignant lung cancers on chest X-rays.
- Researchers analyzed 800 X-rays from four participating centers, including 200 normal chest scans and 600 with at least one malignant lung nodule.
- The average sensitivity, or the ability to detect an existing cancer, improved significantly from 65.1% for radiologists reading alone to 70.3% when assisted by the software.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Dionna Arnold
1-630-590-7791
darnold@rsna.org
OAK BROOK, Ill. — Radiologists assisted by deep-learning based software were better able to detect malignant lung cancers on chest X-rays, according to research published in the journal Radiology.
{kind=link}
"The average sensitivity of radiologists was improved by 5.2% when they re-reviewed X-rays with the deep-learning software," said Byoung Wook Choi, M.D., Ph.D., professor at Yonsei University College of Medicine, and cardiothoracic radiologist in the Department of Radiology in the Yonsei University Health System in Seoul, Korea. "At the same time, the number of false-positive findings per image was reduced."
Dr. Choi said the characteristics of lung lesions including size, density, and location make the detection of lung nodules on chest X-rays more challenging. However, machine learning methods, including the implementation of deep convolutional neural networks (DCNN), have helped to improve detection.
Deep learning is a type of artificial intelligence that allows computers to complete tasks based on existing relationships of data. A DCNN, modeled after brain structure, employs multiple hidden layers and patterns to classify images.
In this retrospective study, radiologists randomly selected a total of 800 X-rays from four participating centers, including 200 normal chest scans and 600 with at least one malignant lung nodule confirmed by CT imaging or pathological examination (50 normal and 150 with cancer from each institution). There were 704 confirmed malignant nodules in the lung cancer X-rays (78.6% primary lung cancers and 21.4% metastases). The majority (56.1%) of the nodules were between 1cm and 2cm, while 43.9% were between 2cm and 3cm.
A second group of radiologists, including three from each institution, interpreted the selected chest X-rays with and without cancerous nodules. The readers then re-read the same X-rays with the assistance of DCNN software, which was trained to detect lung nodules.
The average sensitivity, or the ability to detect an existing cancer, improved significantly from 65.1% for radiologists reading alone to 70.3% when aided by the DCNN software. The number of false positives—incorrectly reporting that cancer is present—per X-ray declined from 0.2 for radiologists alone to 0.18 with the help of the software.
"Computer-aided detection software to detect lung nodules has not been widely accepted and utilized because of high false positive rates, even though it provides relatively high sensitivity," Dr. Choi said. "DCNN may be a solution to reduce the number of false positives."
"Deep Convolutional Neural Network-based Software Improves Radiologist Detection of Malignant Lung Nodules on Chest Radiographs." Collaborating with Dr. Choi were Yongsik Sim, M.D., Myung Jin Chung, M.D., Elmar Kotter, M.D., Sehyo Yune, M.D., Myeongchan Kim, M.D., Synho Do, Ph.D., Kyunghwa Han, Ph.D., Hanmyoung Kim, M.S., Seungwook Yang, Ph.D., and Dong-Jae Lee, Ph.D. The study was funded by Samsung Electronics.
Radiology is edited by David A. Bluemke, M.D., Ph.D., University of Wisconsin School of Medicine and Public Health, Madison, Wis., and owned and published by the Radiological Society of North America, Inc. (http://radiology.rsna.org/)
RSNA is an association of over 53,400 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on X-rays and lung cancer screening, visit RadiologyInfo.org.
Images (.JPG and .TIF format)
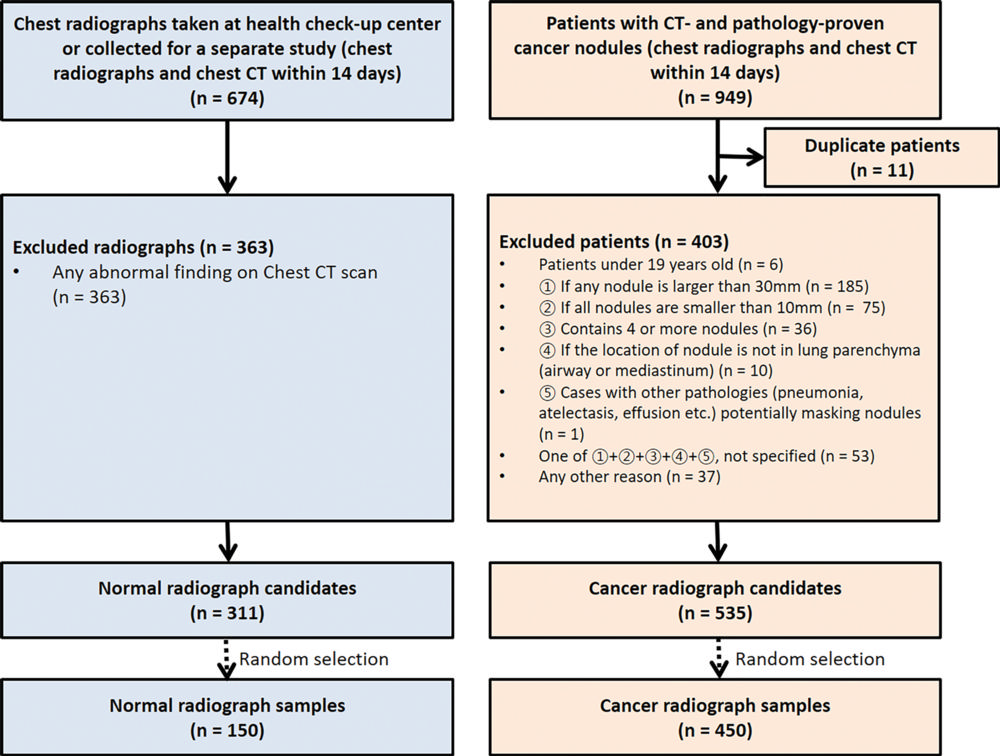
Figure 1. Flowchart of radiograph selection (center 3 not included).
High-res (TIF) version
(Right-click and Save As)
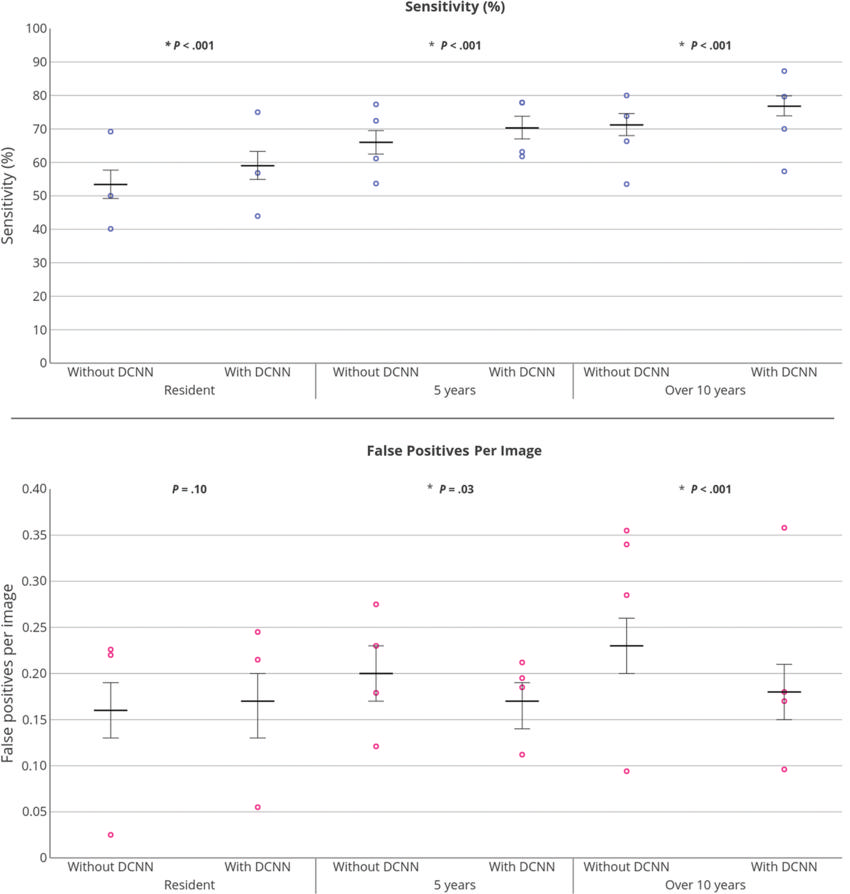
Figure 2. Graphs show results of subgroup performance analysis based on readers' experience. DCNN = deep convolutional neural network.
High-res (TIF) version
(Right-click and Save As)
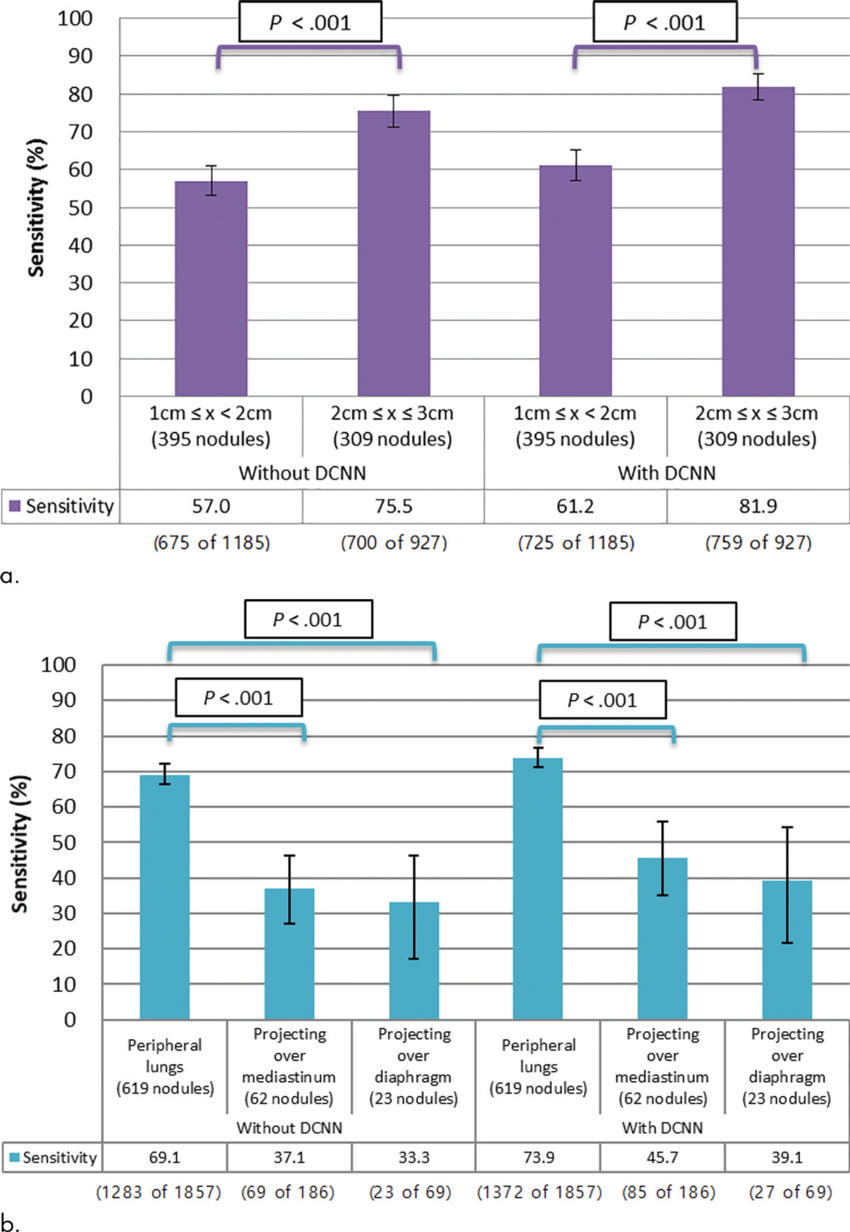
Figure 3. : Graphs show sensitivities and P values when nodules are grouped by size, location, and type. (a) Sensitivities and P values when nodules are grouped by size. (b) Sensitivities and P values when nodules are grouped by location. This shows that the improvement in nodule detection is primarily due to better recognition of the known trouble areas of the posteroanterior chest radiograph (eg, projecting over the mediastinum and diaphragm) (Fig 3 continues).
High-res (TIF) version
(Right-click and Save As)

Figure 3 (continued). Graphs show sensitivities and P values when nodules are grouped by size, location, and type. (c) Sensitivities and P values when nodules are grouped by type. (d) P values for the interaction effects between the use of deep convolutional neural network (DCNN) software and each factor.
High-res (TIF) version
(Right-click and Save As)
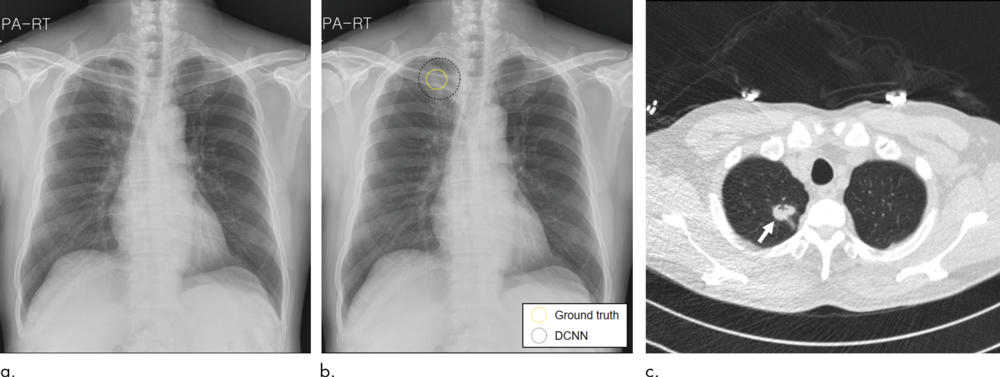
Figure 4. Images in 62-year-old man with primary adenocarcinoma. (a, b) Posteroanterior (PA) digital chest radiographs. (a) Without deep convolutional neural network (DCNN) software assistance, the three readers (readers 10, 11, and 12) interpreted this image as a normal chest radiograph. (b) According to the DCNN's suggestion (dotted circle), all readers were able to identify a true nodule (yellow circle). (c) Axial CT image obtained on the same day shows a 25-mm solid mass in the apical segment of the right upper lobe (arrow).
High-res (TIF) version
(Right-click and Save As)
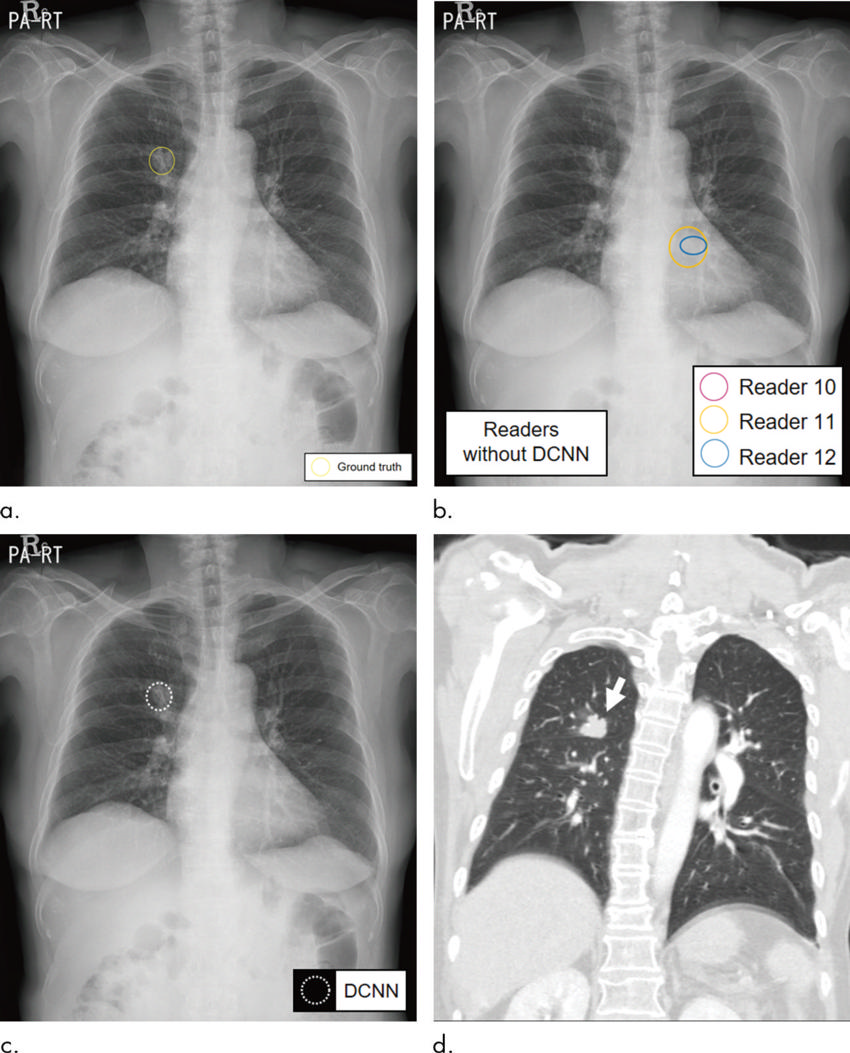
Figure 5. Images in 70-year-old woman with primary adenocarcinoma. (a–c) Posteroanterior (PA) digital chest radiographs. (a) Ground-truth mass (yellow circle) is located in the right middle lung zone. (b) Reader 11 (orange circle) and reader 12 (green circle) marked false-positive regions of interest (ROIs) in the left retrocardiac space instead of the true lesion. Reader 10 initially interpreted this image as normal. (c) With deep convolutional neural network (DCNN) software assistance (dotted circle), all three readers could correctly identify the true nodule in the right lung and abandon their false-positive ROIs. (d) Coronal reconstructed CT image obtained the following day shows a 25-mm mass in the right upper lobe (arrow).
High-res (TIF) version
(Right-click and Save As)