Novel Technique to Treat Endometrial Cysts is Safe and Effective
Released: August 28, 2018
At A Glance
- Researchers evaluated catheter-directed sclerotherapy in 14 patients—ages 20 to 44—with ovarian endometriomas.
- The cysts decreased on average from 5.8 cm in diameter to 1.1 cm, Pain was relieved in all patients, and blood tests indicated well-preserved ovarian function.
- There were no recurrences.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Dionna Arnold
1-630-590-7791
darnold@rsna.org
OAK BROOK, Ill. — A technique called catheter-based sclerotherapy is a safe and effective treatment for endometrial cysts and could help preserve fertility in patients, according to a study appearing in the journal Radiology.

{kind=link}
Endometriosis occurs when the lining of the uterus, known as the endometrium, grows outside of the uterus and into surrounding tissues and organs. It is a common condition that affects about 10 percent of women of reproductive age. When endometriosis involves the ovaries, fluid-filled cysts called endometriomas may form, causing pelvic pain and abnormal uterine bleeding.
Surgery is a common treatment for endometriomas, but it carries risks, including the removal of healthy ovarian tissue, which can affect fertility. Needle-based sclerotherapy is a less-invasive option that involves inserting a needle into the cyst under ultrasound guidance and then withdrawing the cystic fluid through a needle. The cyst is then washed with a solution of ethanol. However, the needle-directed approach has limitations, said study co-author Man-Deuk Kim, M.D., Ph.D., professor at Severance Hospital, Yonsei University College of Medicine in Seoul, South Korea.
"Endometrial cyst content can be incredibly thick and sticky. A 16- or 18-gauge needle, which is commonly used for needle-directed sclerotherapy, is sometimes not large enough to completely evacuate the cyst," he said. "This may reduce the efficacy of sclerotherapy and increase the possibility of needle displacement during aspiration."
Dr. Kim and colleagues studied a sclerotherapy technique that replaces the needle with a catheter, a flexible tube used for removing fluid from cavities in the body. Along with draining cystic fluid more easily, a catheter allows for positional changes during the procedure, which helps maximize the ethanol's effectiveness by enabling it to contact the cyst wall evenly. The catheter also reduces the risk of spillage into the peritoneal cavity of the abdomen.
The researchers evaluated catheter-directed sclerotherapy with 95 percent ethanol in 14 women between the ages of 20 and 44 with ovarian endometriomas.
After about one year, the cysts had decreased on average from 5.8 centimeters (cm) in diameter to 1.1 cm. Pain was relieved in all patients, and blood tests indicated well-preserved ovarian function. There were no procedure-related complications.
There were no endometrioma recurrences, even in patients with internal septation, or division, within their cysts. The multiple compartments of septated cysts can be difficult to puncture with a needle, which may lead to incomplete sclerotherapy. In catheter-directed sclerotherapy, once the endometrioma is punctured, clinicians can manipulate the guidewire and catheter to break down internal septations, allowing for more effective treatment.
"In our study, the recurrence rate of catheter-directed sclerotherapy was 0 percent, which is very encouraging given that endometriomas measuring up to 13.5 centimeters in diameter or those that had internal septation were included in the study," Dr. Kim said.
The results suggest that catheter-based sclerotherapy could lead to better short-term clinical outcomes in women with endometrial cysts while preserving ovarian function and improving future fertility, Dr. Kim noted.
The researchers plan to conduct a study to see how catheter-directed sclerotherapy compares with surgery in terms of fertility, cyst recurrence and improvements in clinical symptoms.
"I hope our catheter-directed sclerotherapy will help women avoid surgery while maintaining ovarian reserve and fertility," Dr. Kim said.
"Catheter-directed Sclerotherapy for Ovarian Endometrioma: Short-term Outcomes." Collaborating with Dr. Kim were Kichang Han, M.D., Seok Kyo Seo, M.D., Gyoung Min Kim, M.D., Joon Ho Kwon, M.D., Hee Joon Kim, M.D., Jong Yun Won, M.D., and Do Yun Lee, M.D.
Radiology is edited by David A. Bluemke, M.D., Ph.D., University of Wisconsin School of Medicine and Public Health, Madison, Wis., and owned and published by the Radiological Society of North America, Inc. (http://radiology.rsna.org/)
RSNA is an association of over 54,200 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on women's imaging, visit RadiologyInfo.org.
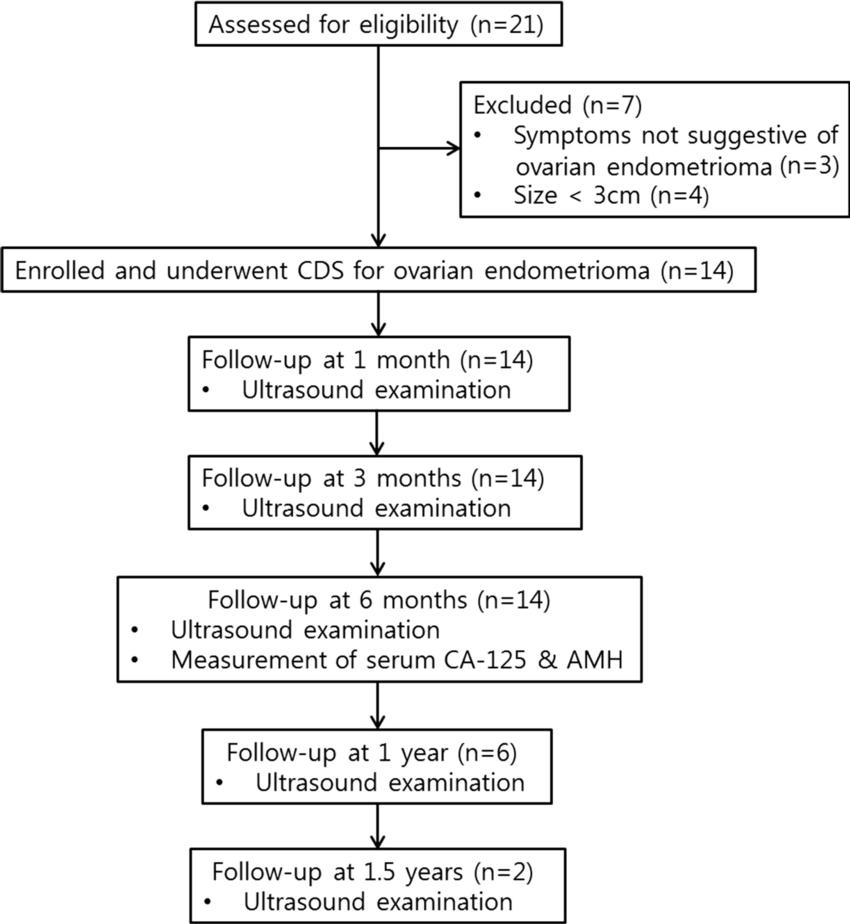
Figure 1. Flowchart for selection of participants for the study. CDS = catheter-directed sclerotherapy, CA-125 = cancer antigen 125, AMH = anti-Müllerian hormone.
High-res (TIF) version
(Right-click and Save As)

Figure 2. Clinical course of a 27-year-old woman with primary ovarian endometrioma presenting with dysmenorrhea. (a) Axial T2-weighted image reveals an 8.4-cm, multilocular endometrioma (∗) with internal septation (arrows). (b) The endometrioma was punctured and mechanical breakdown of the internal septa was performed. (c) A catheter was inserted and contrast agent was injected to observe for any leakage. (d) Follow-up ultrasound 6 months after catheter-directed sclerotherapy shows markedly decreased endometrioma (∗) size (1.4 cm).
High-res (TIF) version
(Right-click and Save As)
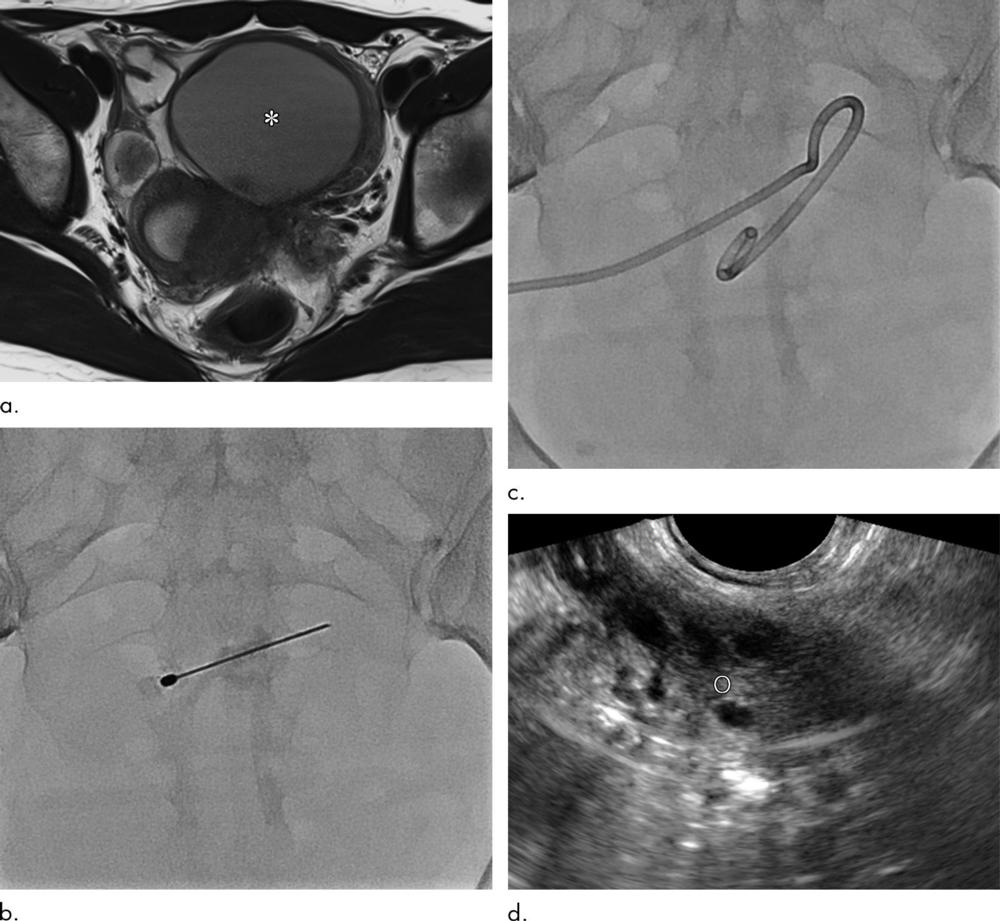
Figure 3. Clinical course of a 30-year-old woman with primary ovarian endometrioma presenting with lower abdominal pain. (a) Axial T2-weighted image shows a 7.1-cm, unilocular endometrioma (∗). (b) The endometrioma was punctured with transabdominal ultrasound (US) guidance. (c) A catheter was inserted and catheter-directed sclerotherapy (CDS) was performed. (d) Follow-up US 6 months after CDS reveals normal-looking ovary (O) without evidence of residual endometrioma.
High-res (TIF) version
(Right-click and Save As)