Imaging Plays Key Role in Evaluating Injuries at Olympics
Released: February 26, 2018
At A Glance
- During the Olympics, onsite imaging services play a critical role in the diagnosis and management of sports injuries and disorders.
- During the 2016 Summer Olympic Games, 1,015 imaging exams were performed on 718 athletes.
- The most common location of injury was the lower limb.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org - Dionna Arnold
1-630-590-7791
darnold@rsna.org
OAK BROOK, Ill. — The Olympic Games give elite athletes a chance at athletic triumph, but also carry a risk of injury. When injuries occur, it is critical that they be evaluated quickly. Onsite imaging services play an important role in the management of Olympic athletes with sports-related injuries and disorders, according to a new study published online in the journal Radiology.

{kind=link}
"The Olympic Summer Games are considered the most important sporting event worldwide. Competing athletes are at the peak of their careers and have trained and practiced for years to be able to participate in the games at a high level," said lead author Ali Guermazi, M.D., Ph.D., professor and vice chair in the Department of Radiology at Boston University School of Medicine, in Boston, Mass., and musculoskeletal radiologist at Boston Medical Center. "Unfortunately, these elite athletes are at risk for injury, and the medical teams onsite will do anything to ensure a fast return to competition or initiate the next appropriate measures in light of more severe injuries."
The Rio de Janeiro 2016 Summer Olympic Games drew more than 11,000 athletes from 206 different countries. During the games, a total of 1,015 radiologic examinations were performed on participating athletes.
"Imaging is paramount for determining whether or not an injured athlete is able to return to competition," Dr. Guermazi said. "Anticipated absence from competition or training is often based on imaging findings. In cases of severe injury, imaging will further help in determining the best therapeutic approach."
Dr. Guermazi and colleagues set out to describe the occurrence of imaging-depicted sports-related stress injuries, fractures, and muscle and tendon disorders, and to document the usage of imaging with X-ray, ultrasound and MRI.
"We wished to elucidate further what types of injuries athletes are incurring, as reflected by imaging, and also emphasize utilization rates of imaging services during the Olympic Games," he said.
The researchers collected and analyzed data from the imaging exams. These data were categorized according to gender, age, participating country, type of sport and body part.
The results showed that 1,101 injuries occurred in 718 of the 11,274 athletes. Of the 1,015 imaging exams performed, 304 (30 percent) were X-ray, 104 (10.2 percent) were ultrasound, and 607 (59.8 percent) were MRI.
"The relevance of imaging is stressed by the fact that a large number of advanced imaging was requested, with MRI comprising nearly 60 percent of all imaging performed for diagnosis of sports-related injuries," Dr. Guermazi said.
Athletes from Europe underwent the most exams with 103 X-rays, 39 ultrasounds and 254 MRIs, but – excluding 10 athletes categorized as refugees – athletes from Africa had the highest utilization rate (14.8 percent). Among the sports, gymnastics (artistic) had the highest percentage of athletes who utilized imaging (15.5 percent), followed by Taekwondo (14.2 percent) and beach volleyball (13.5 percent). Athletics (track and field) had the most examinations (293, including 53 X-rays, 50 ultrasounds and 190 MRIs).
"In some sports, like beach volleyball or Taekwondo, the high utilization rate was somewhat unexpected," Dr. Guermazi said. "These numbers may help in planning imaging services for future events and will also help in analyzing further why some sports are at higher risk for injury and how these injuries can possibly be prevented."
The lower limb was the most common location of imaging-depicted sports-related injuries overall, and imaging of lower extremities was the most common exam. The second most common location was the upper limb.
Among muscle injuries, 83.9 percent affected muscles from the lower extremities. The sports most prone to muscle injuries were athletics, soccer (football) and weightlifting. Athletics also accounted for 34.6 percent of all tendon injuries.
Eighty-four percent of stress injuries were seen in the lower extremities. Stress injuries were most commonly seen in athletics, volleyball, artistic gymnastics and fencing. Fractures were most commonly found in athletics, hockey and cycling. Nearly half were upper extremity fractures.
"Two peaks of imaging utilization were observed, on the fifth and 12th days of the games," Dr. Guermazi said. "This likely corresponds with the timing of judo and athletics events, with both sports showing high proportional utilization rates. These findings will help to plan for increased availability of imaging services during those expected peaks."
Overall, imaging was used to help diagnose sports-related injuries in 6.4 percent of athletes competing in the Olympic Games. High utilization of ultrasound and MRI implies that organizers of future Olympic programs should ensure wide availability of these imaging modalities.
"Imaging continues to be crucial for establishing fast and relevant diagnoses that help in medical decision making during these events," Dr. Guermazi said.
"Sports Injuries at the Rio de Janeiro 2016 Summer Olympics: Use of Diagnostic Imaging Services." Collaborating with Dr. Guermazi were Daichi Hayashi, M.D., Ph.D., Mohamed Jarraya, M.D., Michel D. Crema, M.D., Roald Bahr, M.D., Ph.D., Frank W. Roemer, M.D., Joao Grangeiro, M.D., Richard Budgett, M.D., Torbjorn Soligard, M.D., Ph.D., Romulo Domingues, M.D., Abdalla Skaf, M.D., and Lars Engebretsen, M.D., Ph.D.
Radiology is edited by David A. Bluemke, M.D., Ph.D., University of Wisconsin School of Medicine and Public Health, Madison, Wis., and owned and published by the Radiological Society of North America, Inc. (http://radiology.rsna.org/)
RSNA is an association of over 54,200 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on X-ray, ultrasound, and MRI, visit RadiologyInfo.org.
Images (.JPG and .TIF format)
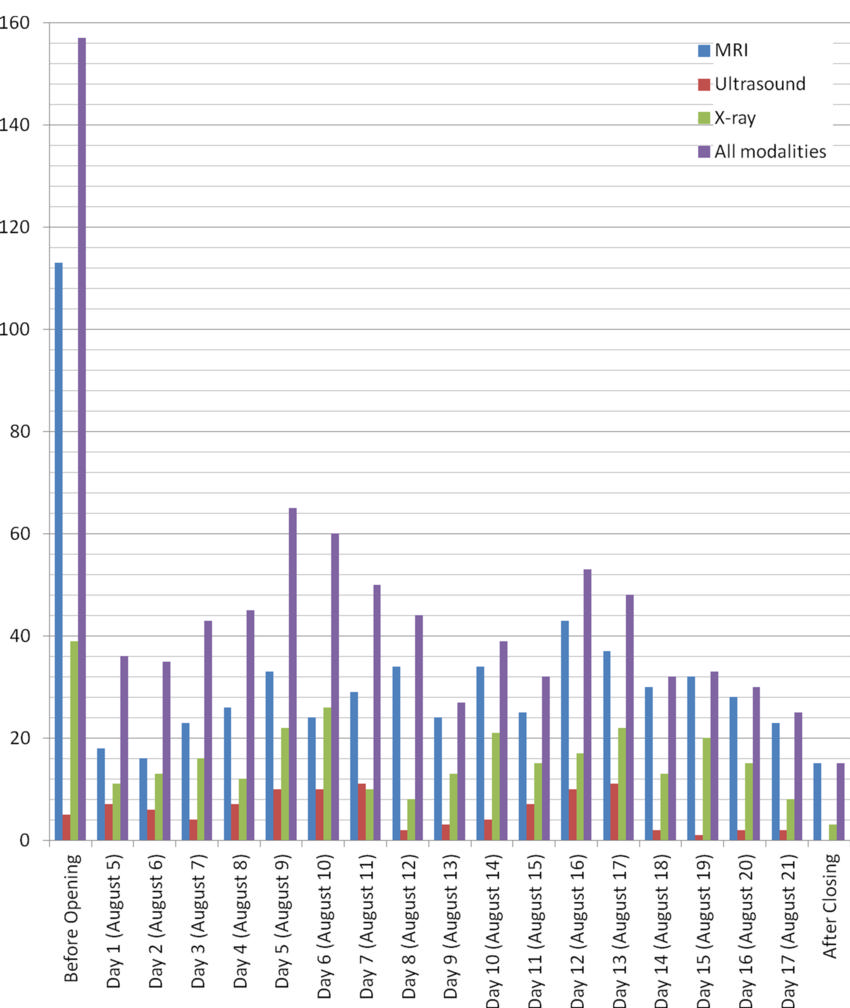
Figure 1. Graph shows distribution of imaging services performed before, during, and after the Rio de Janeiro 2016 Summer Olympic Games.
High-res (TIF) version
(Right-click and Save As)
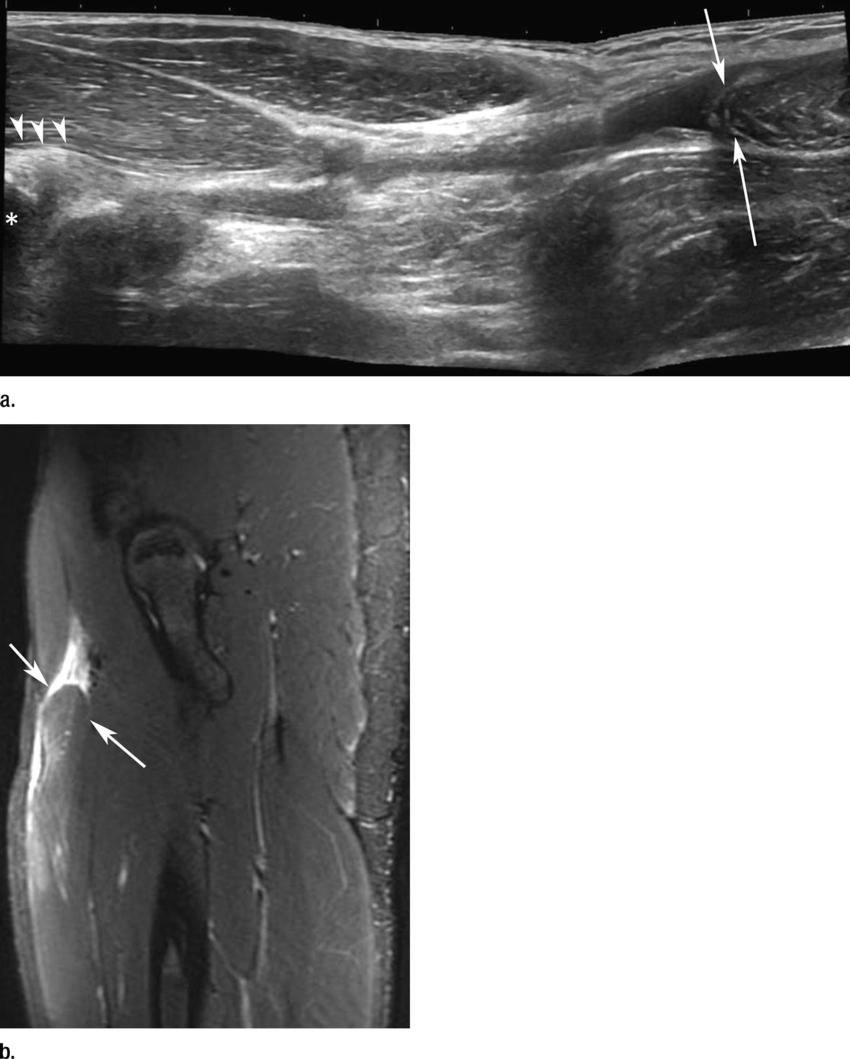
Figure 2. Images in a sprinter with acute anterior thigh pain sustained while training. (a) Ultrasound image of anterior thigh shows complete rupture of proximal rectus femoris muscle (arrowheads) with major distal retraction (arrows). Origin of proximal tendon (arrowheads) is located at anterior inferior iliac spine (∗). (b) Fat-suppressed T2-weighted MR imaging demonstrates distal retraction of proximal rectus femoris muscle (arrows).
High-res (TIF) version
(Right-click and Save As)
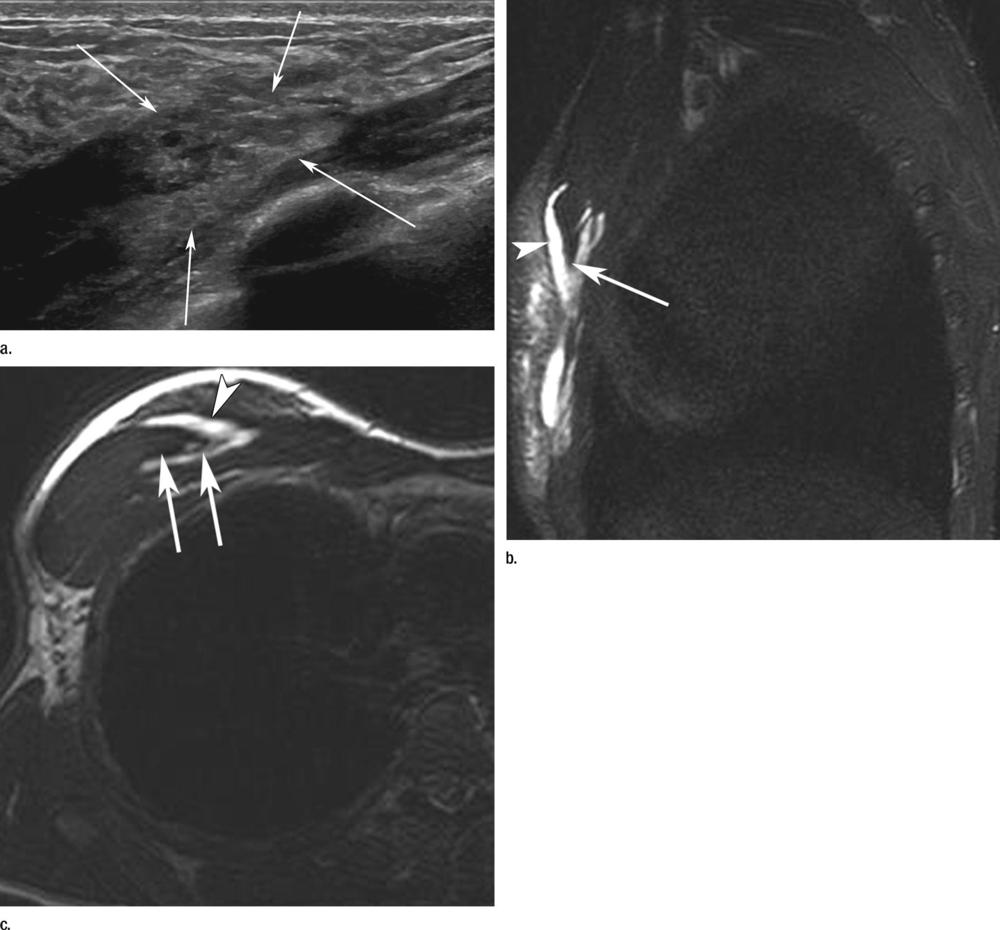
Figure 3. Images in a tennis player with acute pain at anterior chest wall after a match. (a) Ultrasound image of right anterior chest wall shows substantial architectural distortion of proximal aspect of pectoralis major muscle (arrows). (b) Coronal short inversion time inversion-recovery and (c) axial T2-weighted MR imaging was performed in addition to US, and shows major disruption of pectoralis major muscle fibers with intramuscular fluid collection (hematoma, arrowheads) and muscle fibers retraction (arrows).
High-res (TIF) version
(Right-click and Save As)

Figure 4. Images in a long-distance runner with left foot pain without a triggering acute traumatic event. (a) Radiograph of left foot shows fine lucent line in distal diaphysis of third metatarsal representing stress fracture, surrounded by marked periosteal reaction (arrow). (b) Sagittal proton density–weighted MR image of left foot confirms fracture line and periosteal reaction (arrow), and also shows diffuse hyperintensity of entire metatarsal confirming acute nature of stress fracture.
High-res (TIF) version
(Right-click and Save As)

Figure 5. Coronal T1-weighted MR image in road cycling athlete with anterior chest wall pain following direct trauma shows nondisplaced fracture line of sternum (arrow), surrounded by bone marrow edema.
High-res (TIF) version
(Right-click and Save As)
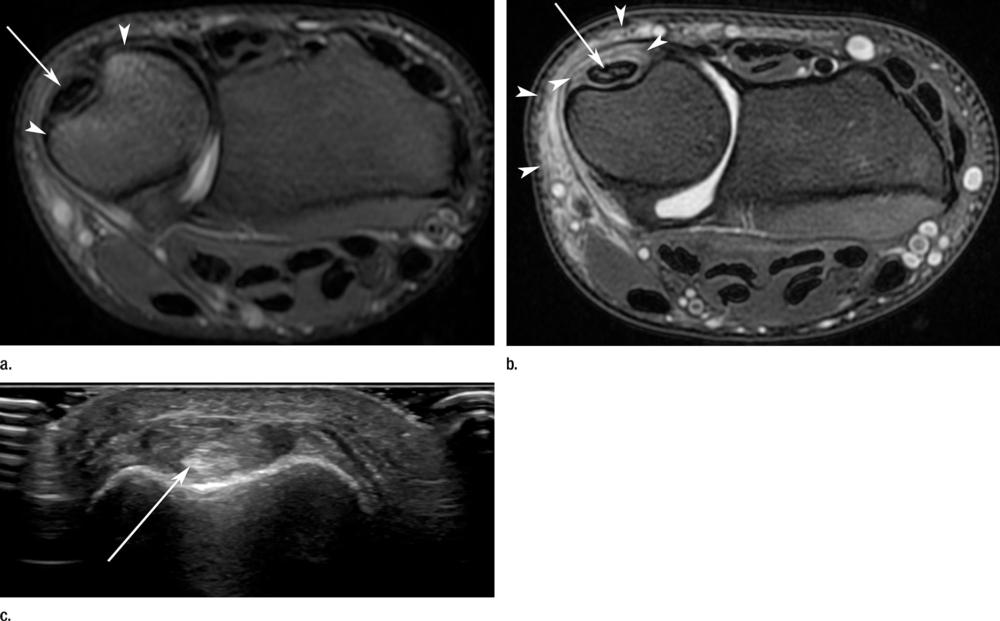
Figure 6. Images in a tennis player with pain at medial side of wrist without a triggering acute traumatic event. (a) Axial T2-weighted MR imaging shows minimal thickening of extensor carpi ulnaris tendon (arrow) with underlying bone marrow edema of ulna (arrowheads). (b) Axial T2-weighted MR imaging 5 days later shows worsening of intratendinous hyperintensity (arrow) with surrounding synovitis and soft-tissue edema (arrowheads). (c) Additional same-day US image shows thickening of extensor carpi ulnaris tendon (arrow) with tenosynovitis.
High-res (TIF) version
(Right-click and Save As)