National Dose Levels Established for 10 Common Adult CT Examinations
Released: February 22, 2017
At A Glance
- Researchers have established diagnostic reference levels (DRLs) and achievable doses for common adult CT examinations.
- Healthcare facilities can optimize these exam protocols so that dose is commensurate with the size of the patient, avoiding unnecessary radiation exposure.
- The use of DRLs has been shown to reduce the overall dose and the range of doses observed in clinical practice.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org

{kind=link}
OAK BROOK, Ill. (Feb. 22, 2017) — Using data from the world’s largest CT dose index registry, researchers have established national dose levels for common adult CT examinations based on patient size. Healthcare facilities can optimize these exam protocols so that dose is commensurate with the size of the patient, avoiding unnecessary radiation exposure.
Results of the two-year study published online in the journal Radiology established patient-size based diagnostic reference levels (DRLs) and achievable doses (ADs) for the 10 most common CT head, neck and body examinations.
While the impact of patient size on radiation dose is well established, national DRLs previously provided only one value for each examination based on a standard-size phantom representing an average patient, a single patient size or data averaged across all patient sizes.
For the study, Kalpana M. Kanal, Ph.D., a medical physicist, professor and section chief in diagnostic physics in the Department of Radiology at the University of Washington School of Medicine, Seattle, and colleagues examined actual patient data from the American College of Radiology (ACR) CT Dose Index Registry to develop size-based DRLs that enable healthcare facilities to compare their patient doses with national benchmarks and more effectively optimize CT protocols for the wide range of patient sizes they examine.
“This extensive participation and totally automated complete capture of all patient examinations enabled the development of robust, clinically based national DRLs and ADs,” Dr. Kanal said.
DRLs — benchmarks for radiation protection and optimization in imaging — were first mentioned in 1990 by the International Commission on Radiological Protection, while the concept of ADs was introduced in 1999 by the United Kingdom National Radiation Protection Board to further optimize CT protocols.
Decades later, there are few national recommendations for DRLs and ADs, mainly because a large volume of robust patient data on CT examinations didn’t exist until the ACR launched its Dose Registry Index in 2011. As of 2016, the ACR registry includes more than 30 million examinations from over 1,500 facilities.
In their research, Dr. Kanal and colleagues accessed more than 1.3 million ACR CT Dose Index Registry examinations conducted in 2014 at 538 healthcare facilities throughout the U.S., located in primarily metropolitan and suburban areas as well as community hospitals.
For head examinations, researchers used lateral thickness as an indicator of patient size, while water-equivalent diameter was used for neck and body examinations.
Data from the 1.3 million CT exams provided median values, as well as means and 25th and 75th DRL percentiles for CT dose index (CTDIvol), dose-length product (DLP) and size-specific dose estimate (SSDE).
DRLs are typically set at the 75th percentile of the dose distribution from a survey conducted across a broad user base using a specified dose-measurement protocol. ADs are set at the 50th percentile of a dose distribution based on the fact that roughly 50 percent of facilities have already achieved doses at or below this value.
Results demonstrated that the new DRLs are not markedly different from those used in other countries.
The use of DRLs has been shown to reduce the overall dose and the range of doses observed in clinical practice, Dr. Kanal said. In terms of using the benchmarks established in their research, she stresses that DRLs should be used to determine if a facility’s dose indexes are unusually high, and are not to be used as target doses.
“Both ADs and DRLs are provided to encourage facilities to optimize dose to a lower level than that indicated by the DRL,” Dr. Kanal said. “Image quality must be taken into consideration when using DRLs and ADs to evaluate CT protocols on each scanner to determine if protocols are optimized.”
Ideally, facilities should analyze and compare their median and size-grouped dose indexes with the respective size-based ADs and DRLs. If size-grouped dose indexes are not available, they should compare their overall median indexes with the average DRLs and ADs across all patient sizes.
“DRLs and ADs are not intended to be used for comparisons with dose indexes for individual patients,” Dr. Kanal said. “Implementation of DRLs and ADs is most effective if the facility has a system to automatically monitor patient dose indexes so that aggregate results may be evaluated.”
Dr. Kanal and colleagues plan to expand their analysis to include high-dose examinations and various scanner configurations and will develop DRLs and ADs for the pediatric population.
Radiologists, radiation oncologists, medical physicists and other radiology professionals are working together to standardize CT protocols.
“U.S. Diagnostic Reference Levels and Achievable Doses for 10 Adult CT Examinations.” Collaborating with Dr. Kanal were Priscilla F. Butler, M.S., Debapriya Sengupta, Ph.D., Mythreyi Bhargavan-Chatfield, Ph.D., Laura P. Coombs, Ph.D., and Richard L. Morin, Ph.D.
Radiology is edited by Herbert Y. Kressel, M.D., Harvard Medical School, Boston, Mass., and owned and published by the Radiological Society of North America, Inc. (http://pubs.rsna.org/journal/radiology)
RSNA is an association of 54,000 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on CT dose, visit RadiologyInfo.org.
Images (.JPG and .TIF format)
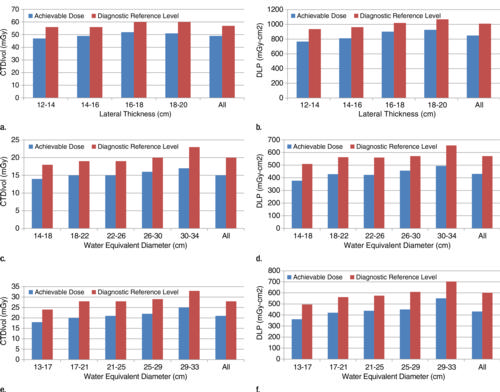
Figure 1. Graphs show head, neck, and cervical spine achievable doses (ADs) and diagnostic reference levels (DRLs). (a) AD and DRL for head and brain without contrast material—volume CT dose index (CTDIvol). (b) AD and DRL for head and brain without contrast material—dose-length product (DLP). (c) AD and DRL for neck with contrast material—CTDIvol. (d) AD and DRL for neck with contrast material—DLP. (e) AD and DRL for cervical spine without contrast material—CTDIvol. (f) AD and DRL for cervical spine without contrast material—DLP.
High-res (TIF) version
(Right-click and Save As)

Figure 2. Graphs show chest achievable doses (ADs) and diagnostic reference levels (DRLs). (a) AD and DRL for chest without contrast material—volume CT dose index (CTDIvol) and size-specific dose estimate (SSDE). (b) AD and DRL for chest without contrast material—dose-length product (DLP). (c) AD and DRL for chest with contrast material—CTDIvol and SSDE. (d) AD and DRL for chest with contrast material—DLP. (e) AD and DRL for chest pulmonary arteries with contrast material—CTDIvol and SSDE. (f) AD and DRL for chest pulmonary arteries with contrast material—DLP.
High-res (TIF) version
(Right-click and Save As)
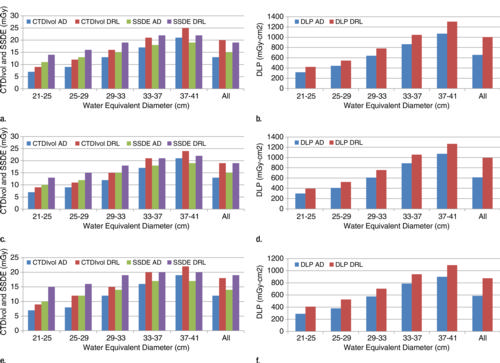
Figure 3. Graphs show abdomen and pelvis achievable doses (ADs) and diagnostic reference levels (DRLs). (a) AD and DRL for abdomen and pelvis without contrast material—volume CT dose index (CTDIvol) and size-specific dose estimate (SSDE). (b) AD and DRL for abdomen and pelvis without contrast material—dose-length product (DLP). (c) AD and DRL for abdomen and pelvis with contrast material—CTDIvol and size-specific dose estimate (SSDE). (d) AD and DRL for abdomen and pelvis with contrast material—DLP. (e) AD and DRL for abdomen, pelvis, and kidney without contrast material—CTDIvol and SSDE. (f) AD and DRL for abdomen, pelvis, and kidney without contrast material—DLP.
High-res (TIF) version
(Right-click and Save As)
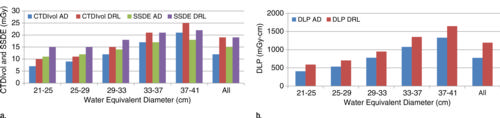
Figure 4. Graphs show chest, abdomen, and pelvis achievable doses (ADs) and diagnostic reference levels (DRLs). (a) AD and DRL for chest, abdomen, and pelvis with contrast material—volume CT dose index (CTDIvol) and size-specific dose estimate (SSDE). (b) AD and DRL for chest, abdomen, and pelvis with contrast material— dose-length product (DLP).
High-res (TIF) version
(Right-click and Save As)
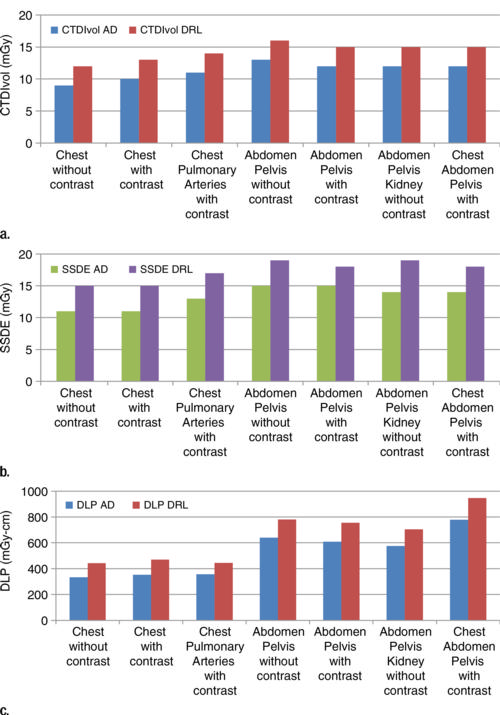
Figure 5. Graphs show achievable dose (AD) and diagnostic reference level (DRL) comparisons for trunk examinations.
High-res (TIF) version
(Right-click and Save As)