Healthcare Reforms Spur Increase in Screening Mammography
Released: September 20, 2016
At A Glance
- Small but significant improvements in mammography utilization were produced under the Medicare Shared Savings Program (MSSP).
- MSSP affords eligible providers, hospitals and suppliers an opportunity to create or participate in Accountable Care Organizations (ACOs).
- ACOs in the MSSP demonstrated a mean increase in mammography screening utilization of 2.6 percent from 2012 to 2014, with 128 of 208 ACOs, or 61.6 percent, reporting improvements.
- RSNA Media Relations
1-630-590-7762
media@rsna.org - Linda Brooks
1-630-590-7738
lbrooks@rsna.org
OAK BROOK, Ill. — The Medicare Shared Savings Program (MSSP) has produced small but significant improvements in mammography utilization in its first three years, according to a new study published online in the journal Radiology.
Established as part of the Affordable Care Act (ACA), MSSP is intended to improve the quality of care for Medicare Fee-For-Service beneficiaries while reducing unnecessary costs. The program affords eligible providers, hospitals and suppliers an opportunity to create or participate in Accountable Care Organizations (ACOs)—groups of doctors, hospitals and other health care providers who work together voluntarily to provide care to their Medicare patients. MSSP represents the largest value-based population reimbursement program in U.S. history.
"The ACA encourages experimentation with alternative-payment models like value-based programs," said study lead author Anand Narayan, M.D., Ph.D., from Johns Hopkins Hospital in Baltimore. "In the value-based model, instead of being paid for doing more tests and procedures, providers get fixed payments tied to measures of whether they doing a good job or not."
While these measures are still coming into focus across medicine, mammography is uniquely situated to measure quality with a robust array of measures tracking outcomes of screening studies.
Dr. Narayan and colleagues recently evaluated the impact of MSSP ACOs on mammography screening utilization through a study of Medicare data on women between the ages of 40 and 69 who underwent screening between 2012 and 2014. ACOs in the MSSP demonstrated a mean increase in mammography screening utilization of 2.6 percent from 2012 to 2014, with 128 of 208 ACOs, or 61.6 percent, reporting improvements. The improved screening adherence ran counter to the trend in traditional fee-for-service populations, where mammography screening was unchanged or declined over the same time periods.
"Pay-for-performance incentives in ACOs can facilitate collaboration amongst various stakeholders across the healthcare continuum to improve mammography screening utilization and other key population health metrics, results which will become increasingly relevant as imaging reimbursements transition from fee-for-service to alternative or value-based payment," Dr. Narayan said.
This transition is well underway, Dr. Narayan noted, with the Centers for Medicare and Medicaid Services publicly announcing its intention to deliver the majority of fee-for-service Medicare payments through value-based programs by 2018. He said that the looming deadline makes it imperative that radiologists work actively with other stakeholders to determine and develop effective strategies for improving population-based health.
"In radiology, we can take an active role in working with other clinicians to ensure that people get appropriate preventive health services," Dr. Narayan said. "For instance, if a 50-year-old woman comes in for a screening mammogram, we could check to see if she is following screening recommendations for colorectal cancer, cervical cancer and other conditions."
Further study is needed to determine the specific tactics that the most successful ACOs used to achieve improvements in screening, according to Dr. Narayan.
"While we weren't able to look at specific practices to see what these organizations did, a wide variety of strategies have been discussed," he said. "Many strategies revolve around communications, such as phone calls, letters, group health education sessions, peer counseling and home visits."
Since the ACA began its rollout in 2010, the number of Americans with health insurance has increased, a trend that may further drive mammography utilization. Previous research showed statistically significant improvements in mammography screening after the state of Massachusetts enacted healthcare reform in 2006.
"Screening mammography is associated with having access to the health care system," Dr. Narayan noted. "Women start getting screening mammograms and a wide variety of other preventive health services when they start seeing primary care doctors."
"Impact of Medicare Shared Savings Program Accountable Care Organizations on Screening Mammography: A Retrospective Cohort Study." Collaborating with Dr. Narayan were Susan C. Harvey, M.D., and Daniel J. Durand, M.D.
Radiology is edited by Herbert Y. Kressel, M.D., Harvard Medical School, Boston, Mass., and owned and published by the Radiological Society of North America, Inc. (http://radiology.rsna.org/)
RSNA is an association of more than 54,000 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on screening mammography, visit RadiologyInfo.org.
Images (.JPG and .TIF format)
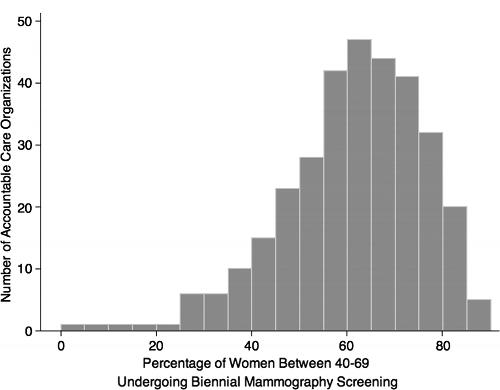
Figure 1. Histogram shows screening mammography use in 333 accountable care organizations in 2014.
High-res (TIF) version
(Right-click and Save As)

Figure 2. Histogram shows differences in screening mammography use from baseline levels in 208 accountable care organizations reporting longitudinal outcomes. There were significant differences in screening mammography use when compared with baseline levels (adjusted IRR, 1.04; 95% CI: 1.02, 1.07; P = .002).
High-res (TIF) version
(Right-click and Save As)